
 |
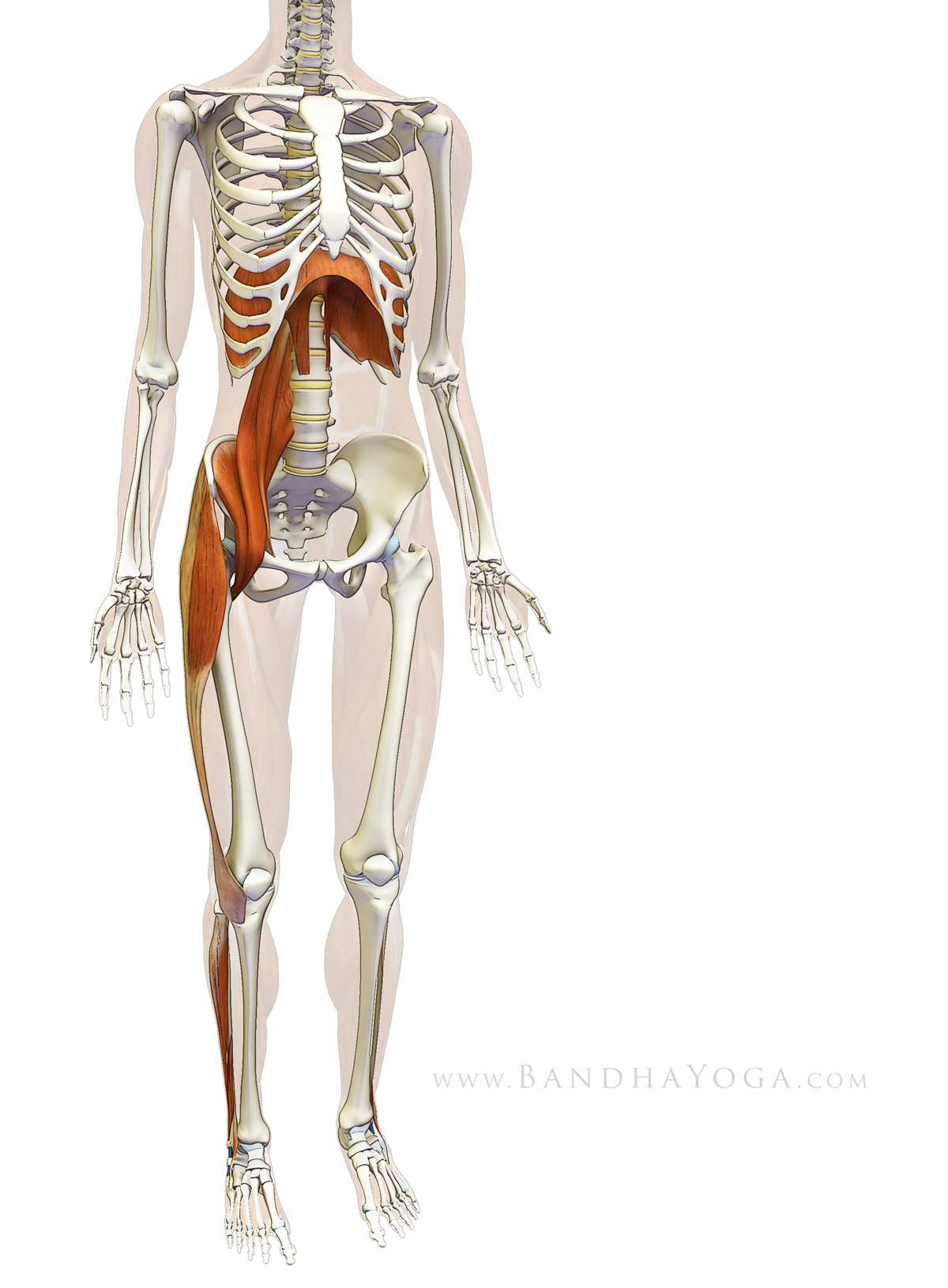
| Figure 1: Myofascial connections between the diaphragm, psoas and lower extremity. |
The diaphragm, as we all know, is the central muscle of breathing. It operates mostly unconsciously, though we can consciously influence its rate and depth of contraction. As the central muscle of breathing the diaphragm is inextricably linked to our life force and thus, our emotions and energetic body. Practicing yoga asanas influences the diaphragm in subtle ways, particularly through its connection to the psoas muscle. In fact, every pose has a slightly different effect on the diaphragm, and thus on its energetic connections.
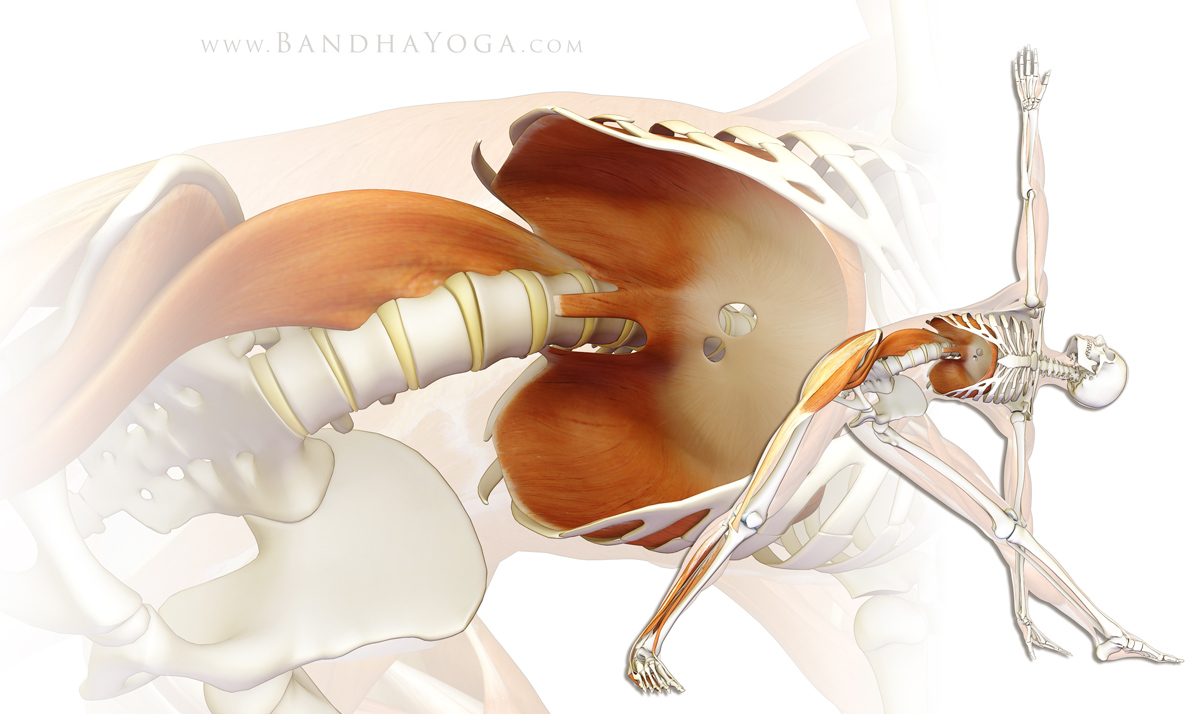 |
| Figure 2: Myofascial connections between the diaphragm, psoas and lower extremity in Trikonasana. |
Visualization is a powerful tool you can use to access these connections. So, before we go on to the details of anatomy and biomechanics, spend a few relaxed moments looking at figures 1 and 2, which illustrate these myofascial connections. Look at the images and then picture the connections within your body (click on the image for a larger view). Repeat this exercise two or three times, devoting five or ten seconds to each visualization. Note how you can feel the connections within yourself. Please complete this process before proceeding with the details of anatomy and biomechanics.
And, here’s the anatomy…
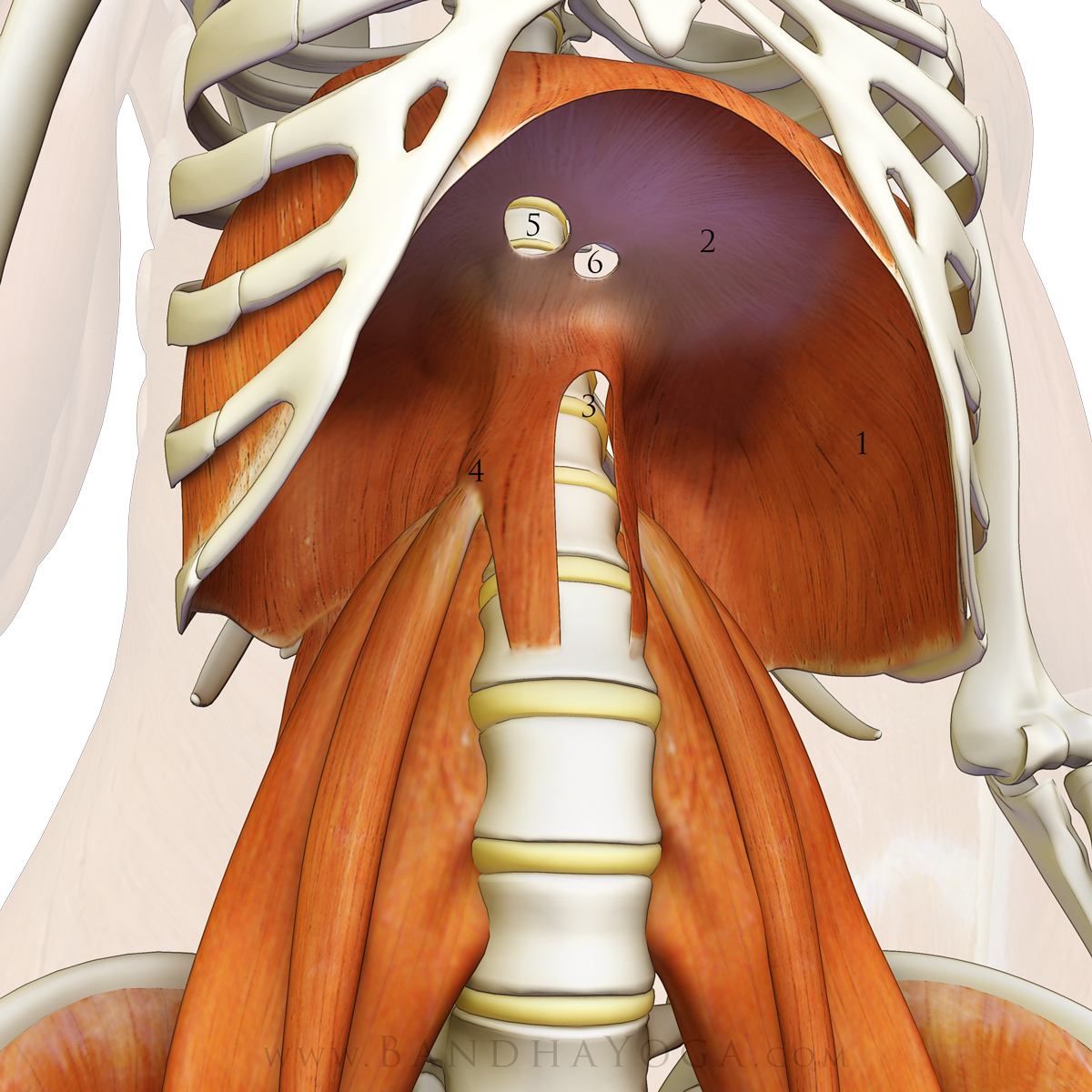
The thoracic diaphragm is a dome shaped muscle that separates the chest and abdominal cavities. The contractile part of this muscle is located peripherally, inserting onto a central tendon (that is not connected to a bone). The origins of the muscle are divided into costal and lumbar portions. The “costal” portion originates from the inner surface of ribs seven through twelve. The “lumbar” portion has both medial (closer to the midline) and lateral (further from the midline) aspects. The medial aspects of the diaphragm arise from the front of the first three lumbar vertebrae (L1-L3). The lateral aspects arise from three tendinous arches. The first tendinous arch is associated with the abdominal aorta, and the second and third with the psoas major and quadratus lumborum muscles respectively. Figure 3 illustrates these structures.
 |
| Figure 3: The diaphragm-psoas connection. 1) diaphragm 2) diaphragm tendon 3) aortic aperture 4) psoas arcade 5) vena caval aperture 6) esophageal aperture |
{kind=link}
Engaging the diaphragm with the glottis open expands the ribcage and produces a pressure gradient by lowering intrathoracic pressure. The negative inspiratory pressure causes air to be drawn into the lungs, thus equalizing the gradient. These fluctuating pressure gradients also facilitate blood flow, particularly venous return to the heart.
Conversely, contracting the diaphragm after exhalation with the glottis closed (as in Nauli) also produces a pressure gradient. In this case the negative inspiratory pressure draws the abdominal contents upwards (and the abdomen in). Engaging the diaphragm on exhalation with the glottis closed is a form of eccentric (or isometric contraction), whereby a muscle is engaged in its lengthened state, but does not shorten.
Engaging the abdominals during exhalation passively stretches the diaphragm by raising the intra-abdominal pressure and lifting the abdominal organs upward against the muscle. Note that engaging the abdominals on exhalation also tensions the thoraco-lumbar fascia, which serves to stabilize the lumbar spine and sacroiliac joint. Click here for more information on this particular connection.
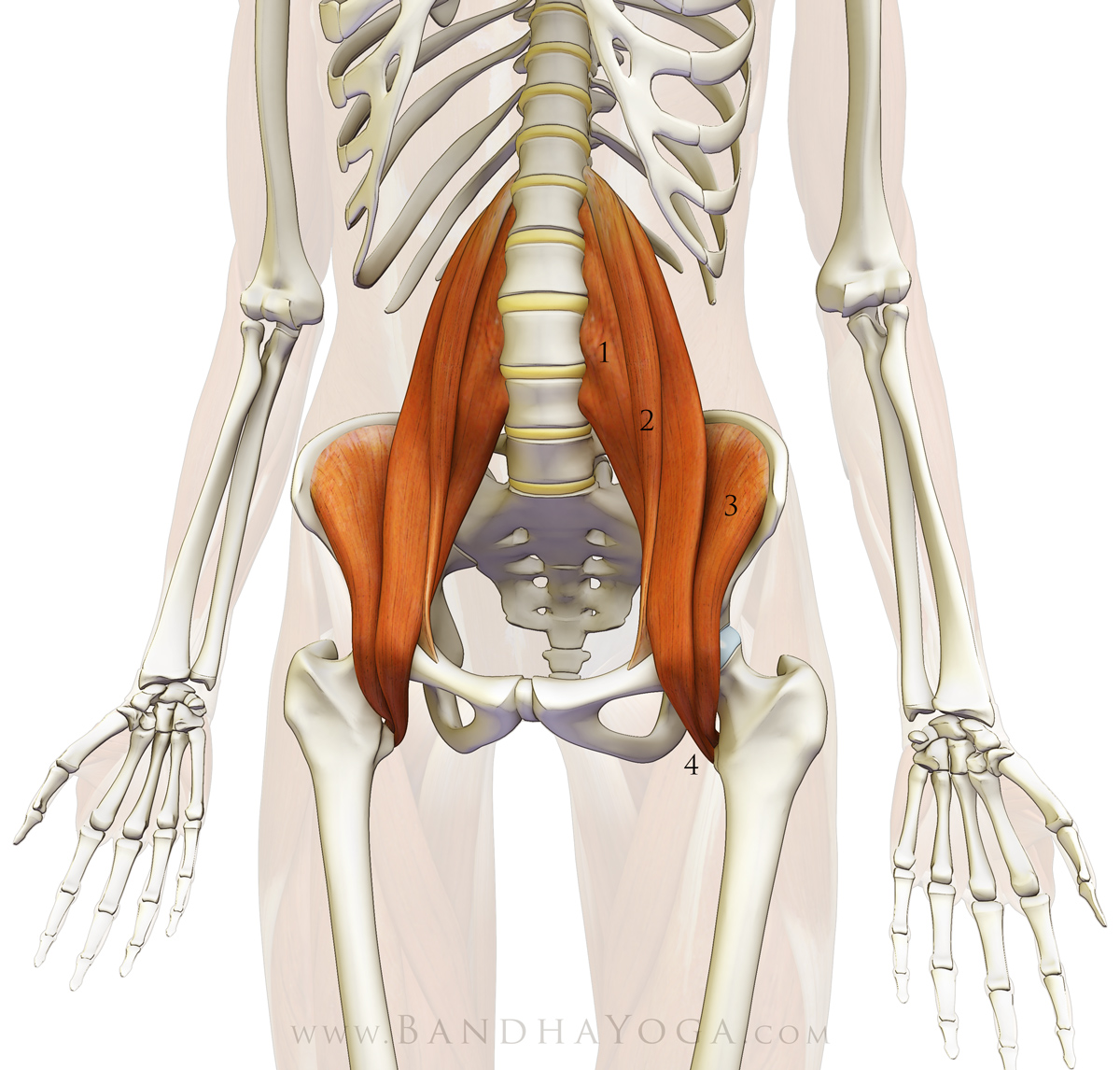
The psoas major muscle originates from the vertebral bodies of T12 and L1 through L4 (lateral surfaces and discs), with a deep layer originating from L1-L5 (costal processes). It combines with the iliacus muscle, which originates from the inside of the ilium (the iliac fossa) to form the iliopsoas muscle. The iliopsoas then runs over the brim of the pelvis to insert onto the lesser trochanter, a knob-like structure on the upper, inside of the femur (thigh bone). The iliopsoas crosses multiple joints and is thus considered a polyarticular muscle. When contracting on one side it can act to flex and externally rotate the femur and/or laterally flex the trunk (as in Trikonasana) or tilt one side of the pelvis forward. When the iliopsoas contracts on both sides it can flex both femurs and the trunk. Bilaterally contracting this muscle lifts the trunk from supine position (lying on the back). Figure 4 illustrates the iliopsoas muscle. Click here for a technique on isolating and awakening this important muscle to use it consciously in yoga poses.
{kind=link}
 |
| Figure 4: The psoas. 1) psoas major 2) psoas minor 3) iliacus 4) iliopsoas (at tendon attachment to the lesser trochanter) |
Now, return to the images illustrating myofascial connection between the diaphragm, the psoas and the lower extremities (figures 1 and 2). Spend a few moments in relaxed visualization of these key structures. Note how your body awareness has deepened in the brief period between now and when you first looked at them. Integrate this process into your daily practice.
Sankalpa and creative visualization are two of the eight components of Yoga Nidra, as described by Swami Satyananda. Though typically performed during the deep relaxation phase of an asana practice, visualization and intent can be worked with during the asanas themselves. Swami Saraswati beautifully describes the process of Sankalpa as a series of stepping-stones that are used to cross a wide river.
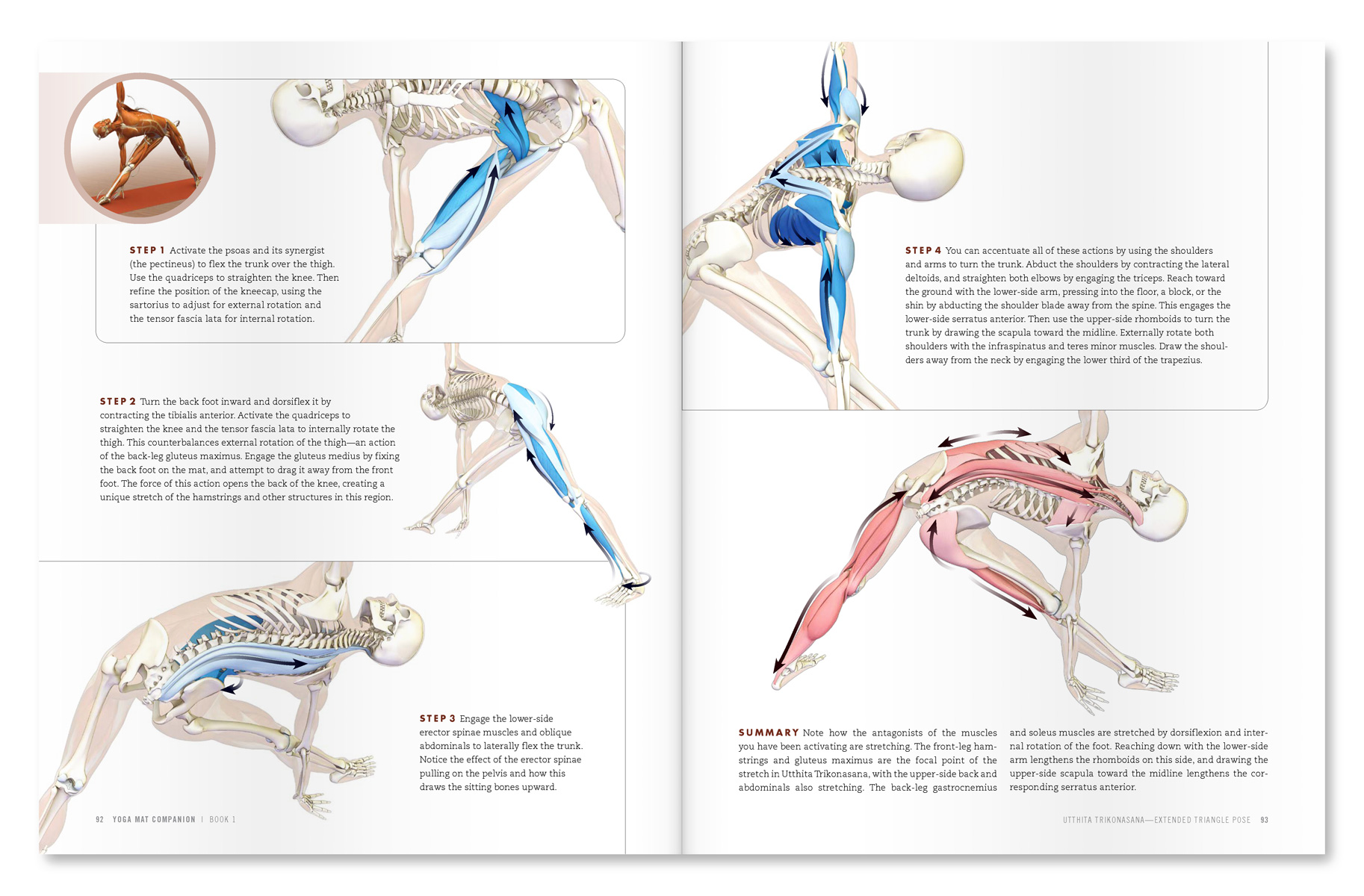 |
| An excerpt from "Yoga Mat Companion 1 - Anatomy for Vinyasa Flow and Standing Poses". |
 |
| An excerpt from "Yoga Mat Companion 1 - Anatomy for Vinyasa Flow and Standing Poses". |
Our books are designed to facilitate this experience. They are based on many years of formal study of anatomy and biomechanics and use carefully designed vivid images that stimulate the visual cortex of the brain, in essence “lighting up” the muscles that are engaging in each part of the body during each pose. In fact, many practitioners say that they can actually “feel” the muscles when looking through The Key Muscles Yoga and The Key Poses of Yoga. The Yoga Mat Companion series deepens this visual experience by illustrating each pose in a step-wise fashion. This visual experience then translates to improvement in your asanas. Click here to page through all of our books.
Namaste’
Ray and Chris
gracias por ten excelente articulo, quisiera saber si el material que venden esta traducido al español,namaste,luna
ReplyDeleteMuchas gracias Nelida - estoy encantado que le guste nuestro trabajo! Usted puede encontrar nuestros libros en español en:
Deletehttp://www.editorialacanto.com/index.php?cat=15&cate=Yoga
Ramon
I simply feel in love for your wonderfull job and great generosity in sharing such a ancien cience in modern views,scientifically perfect.It is dificult to tanks enough.....
DeleteBut I would like to know if there are books traslated in Portuguese.I would like to leave as an important heritage to my 4 children and for my 4 grand children.
Tank your for preetcious time you give to all.
Sorry for my poor English....
Sincerely yours
Maria Victória
You offer so much valuable information! Thank you -- I share it all with my yoga students and yoga teacher trainees!
ReplyDeleteGreat to hear, Peggy. Thank you for sharing it with your students and trainees!
DeleteNamaste'
Ray
impresionante artículo! Gracias por compartirlo!
ReplyDeleteGracias Siempreverde! Ramon
DeleteYour workshop in Costa Rica only will be in english? could be with translation in spanish?
ReplyDeleteHola Siempreverde! Thanks for stopping by. The workshop in Costa Rica is in English. I speak some Spanish, but not enough to give a workshop. We are planning a future workshop in Argentina, where we will have a translator. Best~Ramon
DeleteI would gladly interpret at a future workshop as I could not afford to otherwise. Mil gracias.
DeleteHi, when in Argentina??
ReplyDeleteHi Carola,
DeleteWe don't have a date set on Argentina yet; we'll announce it on the website once it is confirmed. Best~Ray
Any chance of you coming to South Africa? Cape Town?
ReplyDeleteHello Gerda,
DeleteI would love to come to Cape Town at some point. If you know a school that is interested, please have them contact my assistant Carol@bandhayoga.com and we'll arrange it. All the Best~Ray
Thank you so much for sharing this here, as I am too far away to attend the workshops. I really enjoyed reading this article and look forward to seeing your pictures and thoughts about the knee. Namaste
ReplyDeleteThanks Anon--delighted that you enjoy the articles! Ray
DeleteI'm in heaven...this is so beautiful! I will see you in North Carolina next year - I believe in May
ReplyDeleteThanks so much for sharing your wisdom.
My pleasure Ana, many thanks for your compliment on our work! This keeps us going. look forward to seeing you in NC~Ray
DeleteA big Thank you for your generosiy in sharing this information wiht us all!!!, I too am too far away to be able to attend the workshops. I really appreciate reading your articles and look forward to seeing your pictures. Namaste c
ReplyDeleteThank you, Anon! Namaste'~Ray
DeleteThanks for sharing such informative topics. Great.
ReplyDeleteYou're welcome Yoga Guru! Ray
Deletevery useful!thank you
ReplyDeleteThanks Alexandra! Ray
DeleteHi Ray
ReplyDeleteI am new to yoga but love it. I am wondering if a beginner in yoga would struggle in the workshop?
Thanks
Hello Kath,
DeleteWe have beginners to "advanced" practitioners in our workshops. I tailor the asanas to the individuals, everyone learns. Hope to see you! Ray
I have been practicing Yoga off and on for a long time. I love your blog and the beautiful anatomy illustrations. They are extremely helpful and motivated me to buy your books and restart practicing Hatha Yoga.
ReplyDeleteI recently had total hip replacement and because many of the tendons and ligaments to the head of the femur were cut, I cannot perform many of the old asanas that I used to do for fear of popping out the hip joint. I showed my surgeon some illustrations of asanas and asked if I could do these again... His response was "On purpose?"
But in all seriousness, there is a growing segment of the population (like me) who are older and could benefit from Yoga. Can you do some posts or even a book on dealing with joint replacement in practice and how to strengthen the areas so one can do a more full Yoga workout?
Hi Stephen,
DeleteThanks for stopping by. Ask your doc to advise you on the surgical approach he used to replace your hip, the range of motion he recommends and the limitations (partly based on the surgical approach). Tell him the pictures are of yoga, an ancient art that is practiced around the world by millions of people--on purpose (with purpose) to enhance their lives in many ways. You can mention that the American Academy of Orthopedic Surgeons has cited it as one of the adjuncts for conservative management of knee arthritis and you would like to return to it so you can avoid having him replace your knee...:)
Thanks for the suggestion on a post. It's a bit complex and depends on the individual hip replacement (with a number of factors), so I usually tell people to follow their docs restrictions on range of motion and use common sense on which poses they work with. See my blog post on balancing freedom and restraint in yoga. All the Best and good luck on returning to practice! Ray
I wait 4 you soon in Argentina! Thanks 4 this excellent info; are you annoucing in this news letters when are you coming?
ReplyDeleteHi Willie,
DeleteYes, I will announce when we are coming to Argentina. Thank you for your compliment on our work! Ray
This is excellent, the graphics plus the explanations, I love it, many thanks!!
ReplyDeleteThanks Josune! great to hear that you enjoy our work~Ray
DeleteAppreciate the initiative and precious information.. Namaste
ReplyDeleteThanks Yoga Plus! Ray
DeleteRay, in this post you wrote about the myofascial connection between diaphragm, psoas and lower extremity (TFL and peroneus, according to figure 1??). I agree with diafragm-psoas linkage of course, but I don't understand how is it myofascially connected to the external side of the leg, if they don't belong to the same muscular chain? In Uthittha Trikonasana I think that the linkage is made via obliques muscles. Please, could you explain it better. Thank you very much!
ReplyDeleteHi Esperanza,
DeleteThe abdominal obliques are also connected to the muscles of the lower leg--via the periosteum on the iliac crest to the TFL and thence to the other muscles illustrated (and multiple other muscles). I am showing a connection that is deep to that, and also functional. The TFL is connected, also via the periosteum, to the iliacus. If you look at the function of the obliques in a side bend, like Trikonasana, then you can see that they stretch, as does the psoas major (they are synergists for side flexion of the trunk). The TFL synergizes the obliques and the psoas major when coming up from a side bend like Trikonasana (both via closed chain contraction); indeed the linkage shown here from the TFL to the lower leg should be a focus on when coming up from this pose. Using these muscles when coming out of the pose helps to avoid back strain. I'll show the oblique connection in a future post. Thanks for commenting~Ray
Thank you Ray for the detailed explanation. I'm really interested in fascial topics, I couldn't imagine the conecction of deep fascia and the periosteum, that's amazing. I will follow your future post in the blog. I think that biomechanical and anatomical comprehension is essetial for understanding the 'asana' and performing it the best. Thank you for sharing your knowledge!
DeleteI wait with baited breath for these postings. They are so helpful and informative for my own practice and have become invaluable in explaining postures and cues for my classes. I have purchased all the books in the series yet, the postings always seem to follow what I'm working with in my practice and help to convey vital yogic anatomy to the students who attend my classes.
ReplyDeleteThanks Ray and Chris...Namaste!
Awesome to hear, John--delighted that you enjoy our work! Many thanks for your positive feedback as what you describe (helping in your practice and teaching) is our goal. Namaste'~Ray
DeleteThankyou very much for this beautifully written and very informative article.
ReplyDeleteThe illustrations are amazing and very helpful also.
Namaste!
Thank you, Anon! Ray
DeleteThis is my second read through. When I purchased some of your books a few years back I recieved a poster of the iliopsoas. I glued it to a poster board and still have it. I am anxious to get home so I can be "awed".
ReplyDeleteYour post are really worth taking the time to do several reading sessions. There is so much to take in that the second time through was even greater than the first!!!
You WOW us in the way you inform!!! Thanks so much...
Hi Ana,
DeleteMy apologies for the much delayed response to your comment. Many thanks for your compliments-- I very much appreciate your thoughts~Ray
Hi. Love your posts. Is there a chance you will come to Israel for workshop?
ReplyDeleteHi Yamit,
DeleteThanks for your compliments! I would love to come to Israel for a workshop. Please contact my assistant, Carol (carol@bandhayoga.com) if you would like to host one. All the Best~Ray
Wonderful post, but I have a discussion point.An eccentric contraction is one in which the muscle contracts to slow its rate of lengthening. For the diaphragm, this would require something to create a force against its inferior aspect while at the same time the muscle is contracting in a manner to push back against this inferior force but with less force than the one on its inferior aspect.
ReplyDeleteCould this occur when we are inverted, letting the glottis relax, but using the diaphragm to slow exhale ?
Partially closing the glottis on exhale will create a force within the thorax, which the force pushing from the inferior side of the diaphragm must overcome for the diaphragm to fully lengthen. Potentially this allows the diaphragm to let go. In direct opposition to the statement in this post, which is suggesting that the diaphragm is contracting to exert an upward force against the glottis created force, the diaphragm cannot contract and exert a force in a superior direction. It can only decrease superior exerted forces in the thorax, Right?
Maybe we should consider this - wouldn't that be an interesting effect of ujjayi breath? by contracting the abdominals to draw in the abdomen, and contracting the glottis to increase thoracic pressure, might the diaphragm be able to move passively during exhale? would that give it more R&R?
Hi Neil,
DeleteThanks for commenting--very interesting discussion points. I agree that eccentric contraction is typically defined as you describe, i.e. a contraction against a weight that exceeds the contractile force so that the joint angle increases rather than decreases (as with concentric contraction). I think what happens when one closes the glottis after the end of exhalation and then attempts to inhale, the diaphragm develops a contractile force, but probably doesn't have that much excursion. So it wouldn't be a pure eccentric contraction like that typically described for the usual definition. However, I look at eccentric contraction as more of a spectrum that includes the situation where the muscle is engaging when in a lengthened state, but not shortening--could be a type of isometric contraction. The force generated draws the abdominal contents upward, rather than air into the trachea. Could be augmented by engaging the accessory muscles of inspiration (which is what I do myself). But I agree with you that it wouldn't be the typical eccentric contraction and will clarify that. Thanks for pointing it out. I'm jet lagged from travel and just getting to bed, so I want to think about your other points regarding inversions a bit more and will add my thoughts later. I do think that strengthening the diaphragm is one of the benefits of inversions, however. It's a bit like reverse abdominal breathing (where one engages the abs on inhalation, thus raising intra-abdominal pressure). This is a common Qi Gong technique which I've been practicing--great effects. In the case of inversions, the diaphragm has to contract against the weight of the abdominal contents, thus giving it a bit of a work out. Let me think about your other thoughts, as they are more in depth. Thanks again for adding to the discussion. Cheers! Ray
Thank you and wondering if you have any plans in the future to animate the movements? It would be great to see the psoas elongating when bending then coming back to rest.
ReplyDeleteThank you for this--very helpful on the connection between diaphragm and psoas. I'm not an anatomy expert by any means, but I feel I'm getting a handle on it through your posts. After reading this one I'm wondering if you have any advice on how to avoid over using the psoas in Navasana and Padangusthasana? Teachers always tell me to straighten my back or use my core more, but I still find I'm mostly using the hip flexors, and frankly it feels like I'm doing more harm than good in these poses.
ReplyDeleteThanks!
Gracias por la información,
ReplyDeleteSala dharma
Una información muy interesante. En el caso de una persona con el diafragma bloqueado y rígido ¿qué posturas aconsejarías practicar para flexibilizarlo?
ReplyDeletesaludos cordiales
Cristóbal
I often talk of your great posts and share them with my students, this is a great help to me personally, thank you, Suzanne
ReplyDeleteAs always, thank you for sharing, I gave my books to two teachers, will order more ;) I recommend your site to anyone interested in yoga... Each posture with the engaged muscles is so clear, everyone is learning something ;) A major help to enter a posture and benefit from it.
ReplyDeleteSo perfectly done . ☀️🎈
thank you very much for sharing this knowledge
ReplyDeleteGracias por tan buen artículo.
ReplyDeletethank you very much. enlightening as always!
ReplyDeleteGreetings and big Gratitude for all the care you take in creating this excellent information. With respect to this post in particular, I have a question regarding releasing the psoas but in a seated or supine position. I work with a paraplegic who has, as you might expect, incredibly tight hips. The deeper holding in the psoas causes spasms through one of his legs, and though we have made incredible strides in opening this area, working with the deep iliopsoas without the ability to access standing postures has presented quite a challenge. Can you suggest or point me in the direction of information on how my student and I might adapt some of your suggestions to the practice?
ReplyDelete