"God is in the Details"--Ludwig Mies van der Rohe
Attention to detail integrates mindfulness meditation into your Hatha yoga practice, enhancing the benefits. This blog post illustrates a detailed tip for engaging the TFL in the forward bend Upavista konasana, its biomechanical basis and the benefits of utilizing this important muscle in your forward bends.
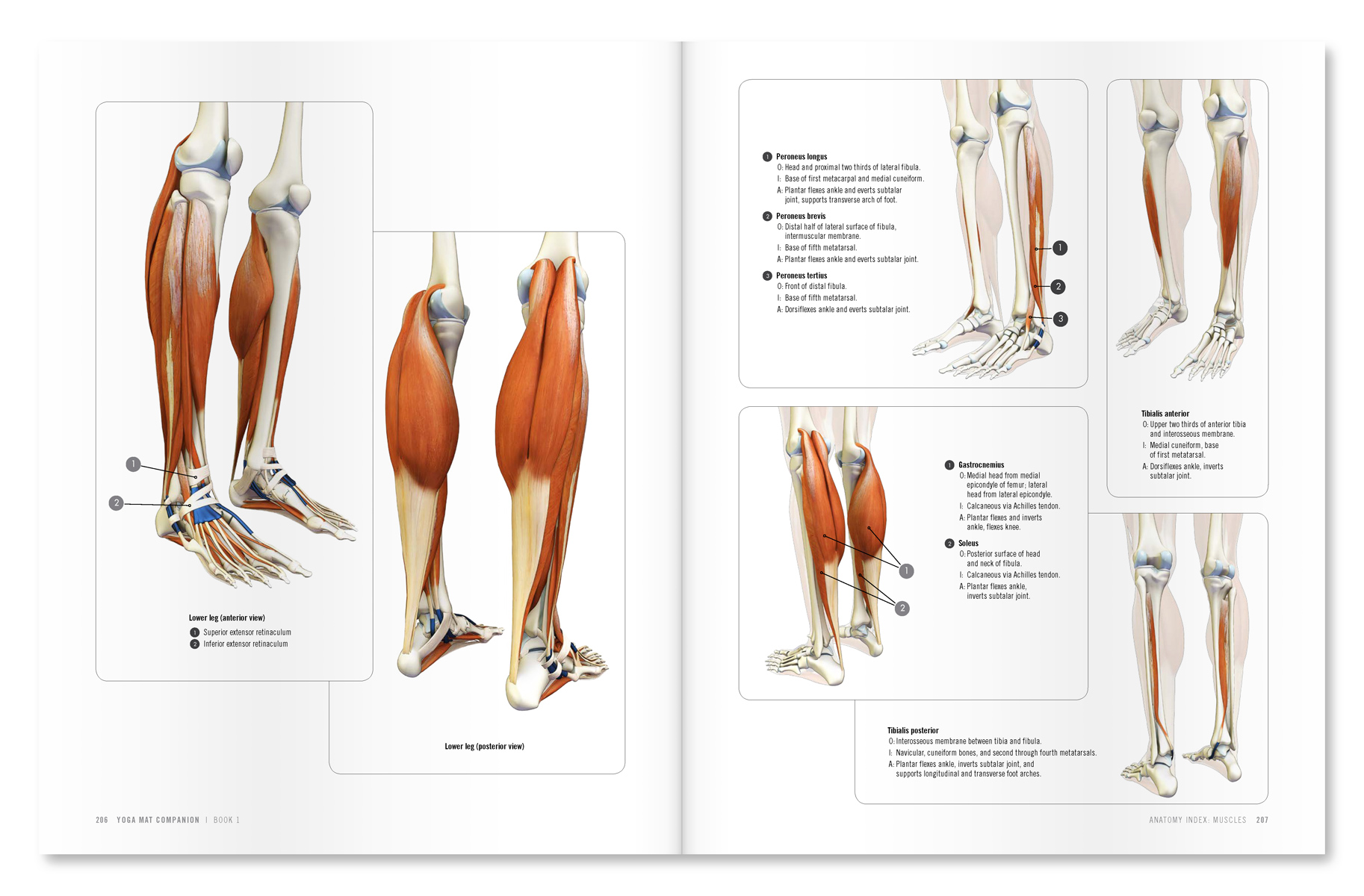
Here’s the anatomy…
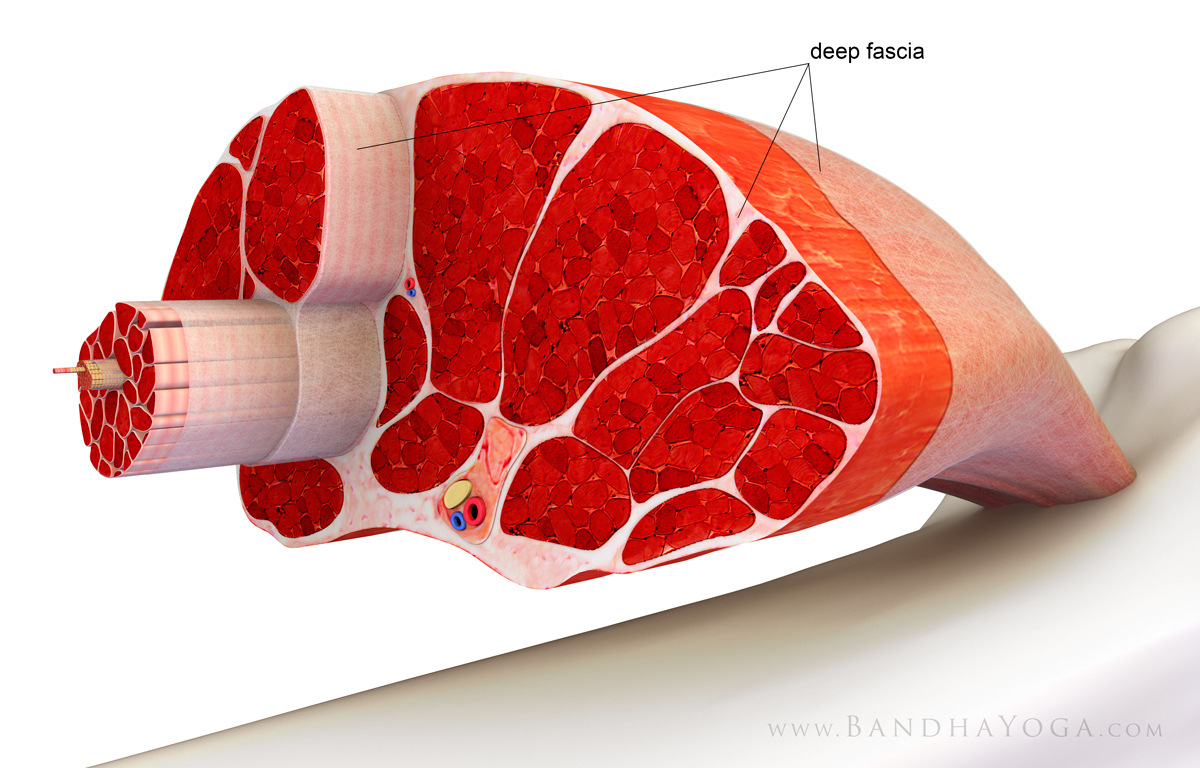
The tensor fascia lata originates from the front part of the iliac crest and outer surface of the anterior superior iliac spine (ASIS). It inserts onto the iliotibial tract (IT band), which continues on to the front outside of the tibia (lower leg bone). It is considered a polyarticular muscle because it crosses both the hip and knee joint. Thus, contracting the TFL can influence both the hips and the knees, as we illustrate below.
Here’s the cue…
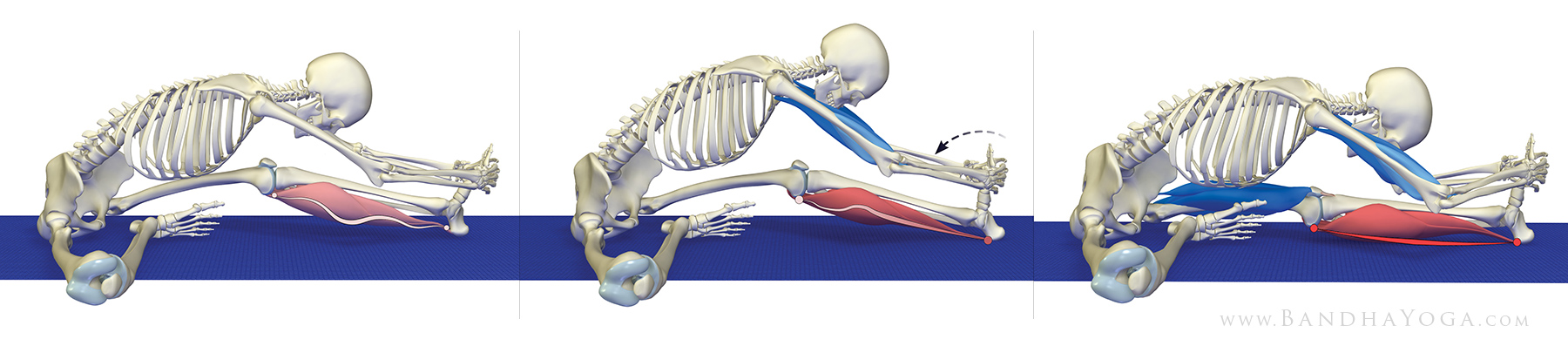
I always begin by taking the general shape of the pose. In the case of Upavista konasana this means taking the legs apart (abduction) and extending the knees. Then I actively engage the quadriceps to straighten the knees. This initiates reciprocal inhibition of the hamstrings, preparing them for the stretch. Next, I bring in the tensor fascia lata (TFL). The cue for this is to press the heels into the mat and then attempt to drag them apart (abduction). This causes the TFL to contract, which you can feel by placing your hands on the sides of the hips as shown below. Pressing the sides of the feet with your hands augments this cue (see figures 1 and 2 below--click on image to enlarge).
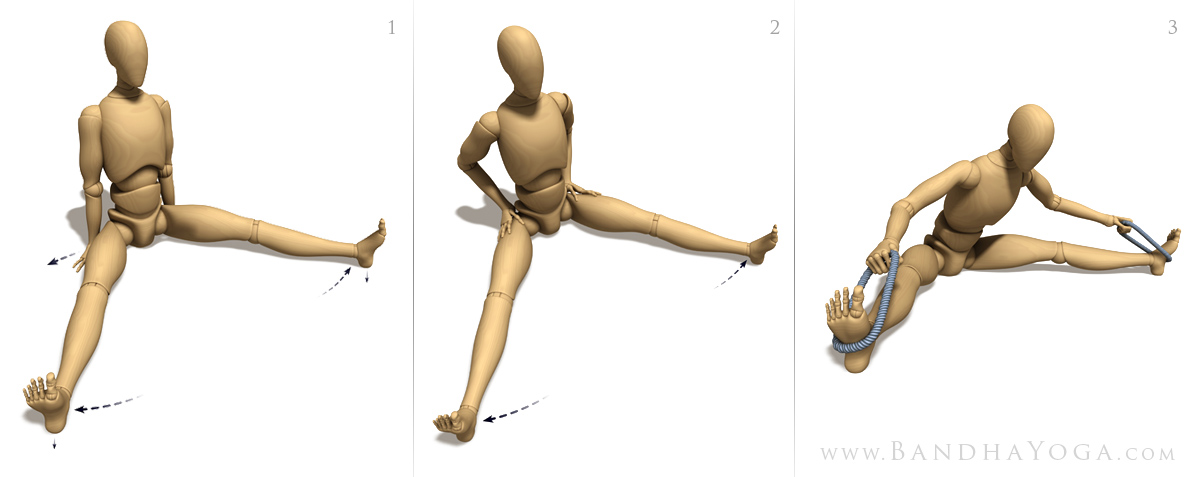 |
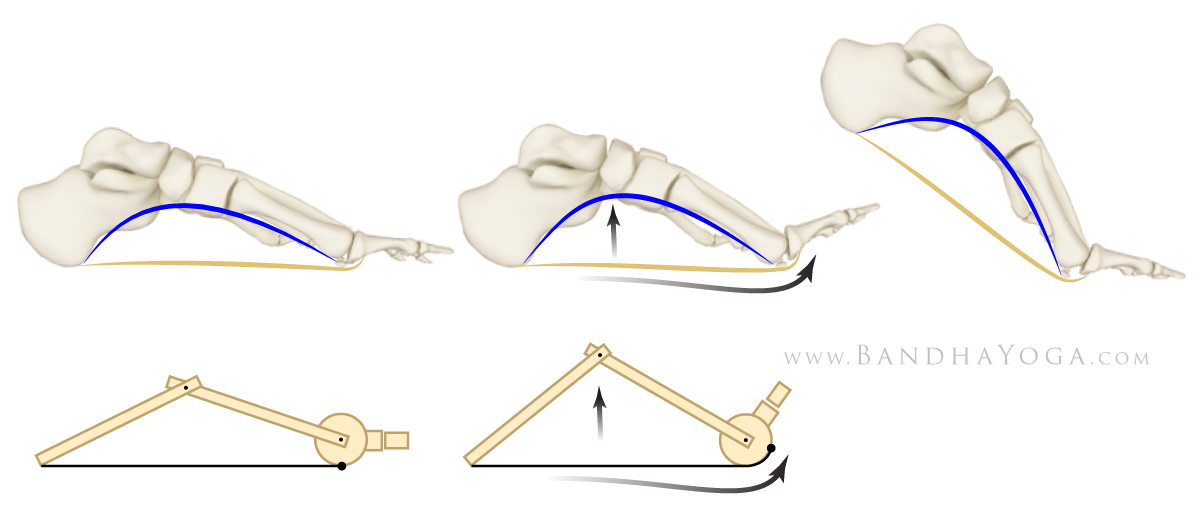
| Figure 1 illustrates pressing the heels down and attempting to drag the feet apart. Figure 2 shows how you can feel the TFL contract. Figure 3 is an intermediate version of the pose. |
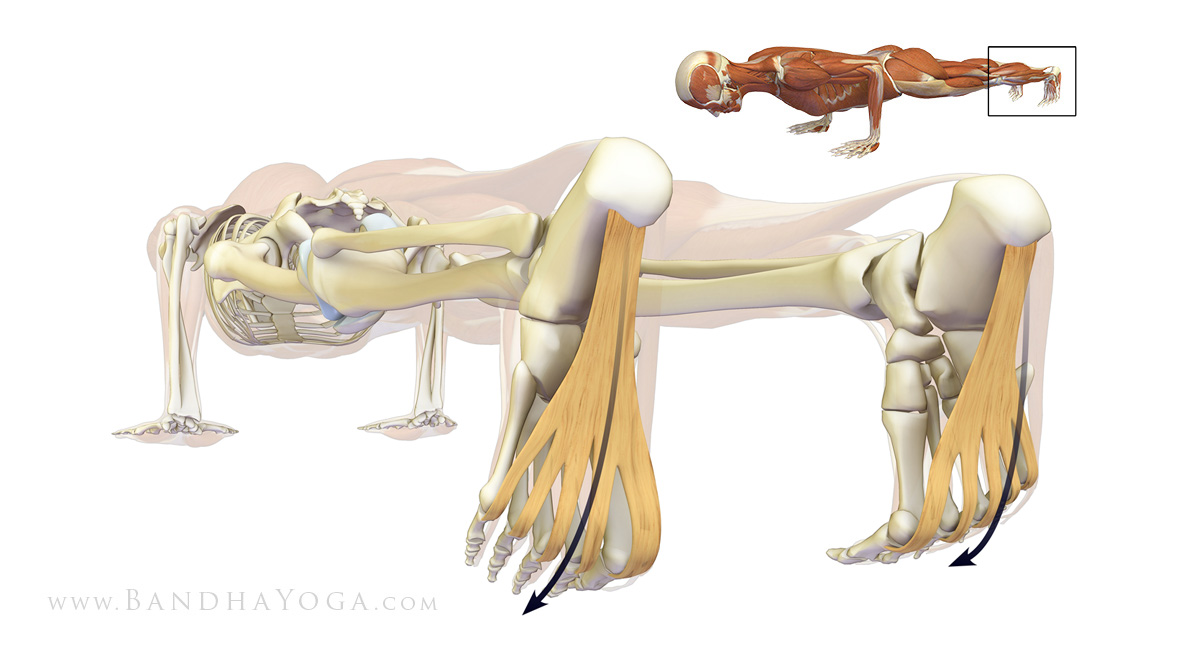
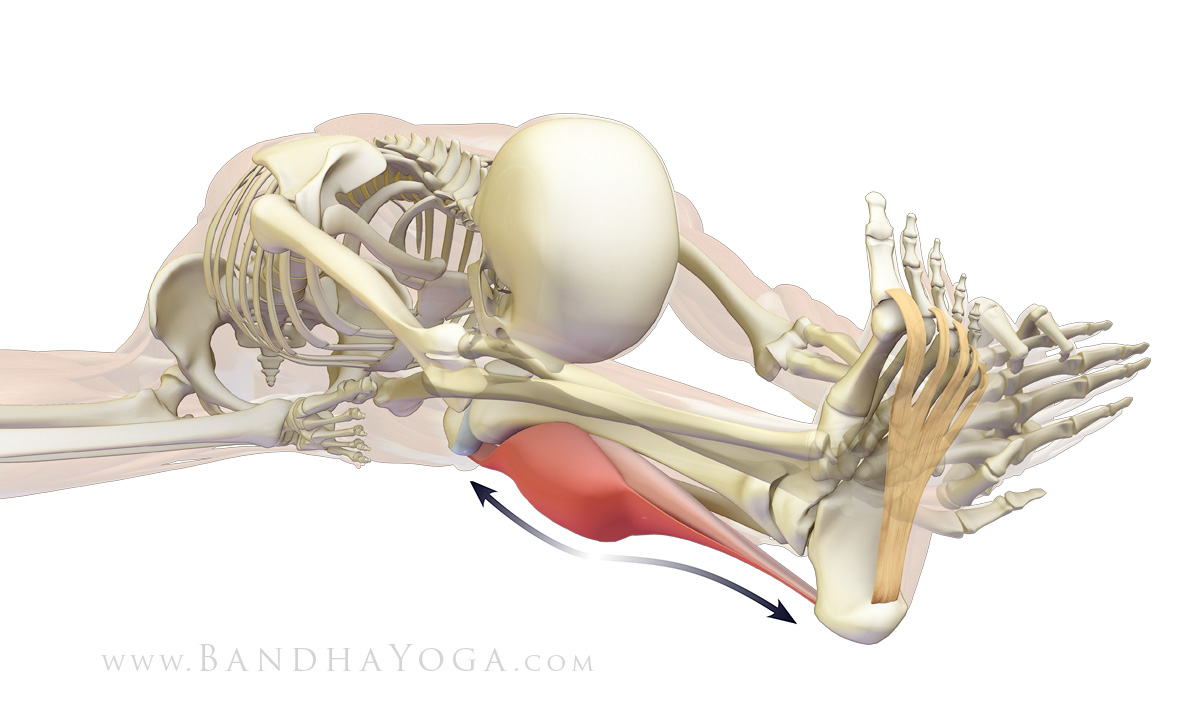
Attempting to drag the feet apart with the heels fixed in place on the mat uses the primary action of the TFL (hip abduction) as a cue to access its secondary actions—knee extension, and hip flexion and internal rotation. Knee extension synergizes the quadriceps and helps to align and protect the knees. Hip internal rotation counteracts the thighs rolling outward as a result of the pull from stretching the gluteus maximus. The TFL synergizes the psoas for hip flexion and contributes to femoral-pelvic and lumbar-pelvic rhythm. You can learn more about the concept of joint rhythm and its effect on the spine from our blog post “Preventative Strategies for Lower Back Strains in Yoga”. Figure 4 illustrates these actions in Uppavishta konasana.
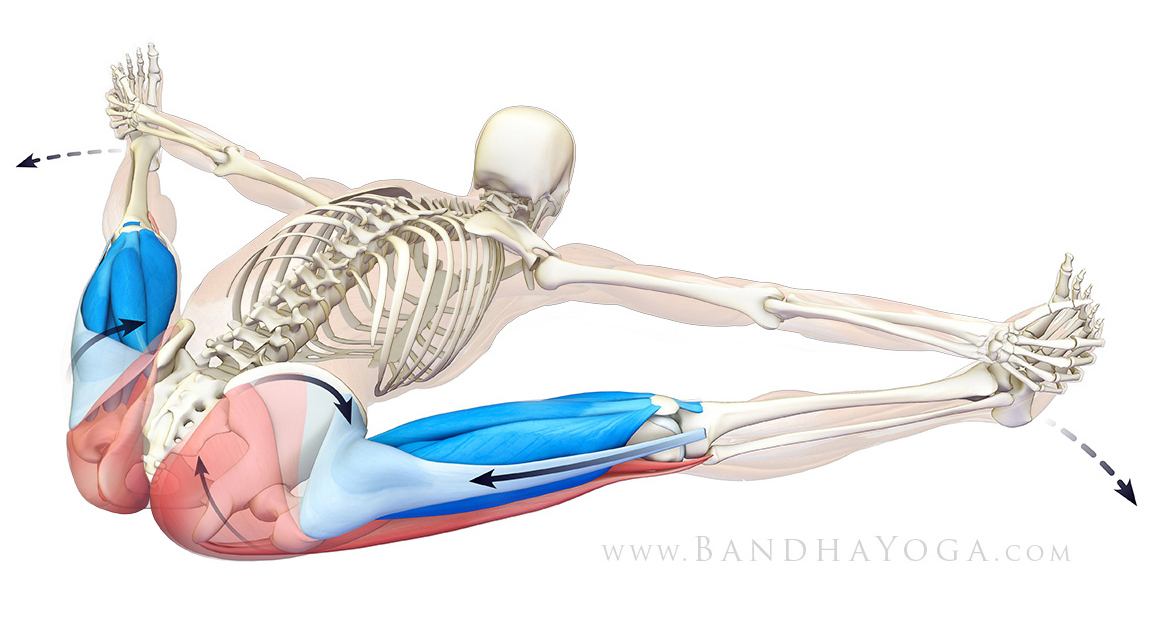 |
| Figure 4 illustrates the action of the TFL on tilting the pelvis forward, internally rotating the thighs and synergizing the quadriceps to extend the knees. |
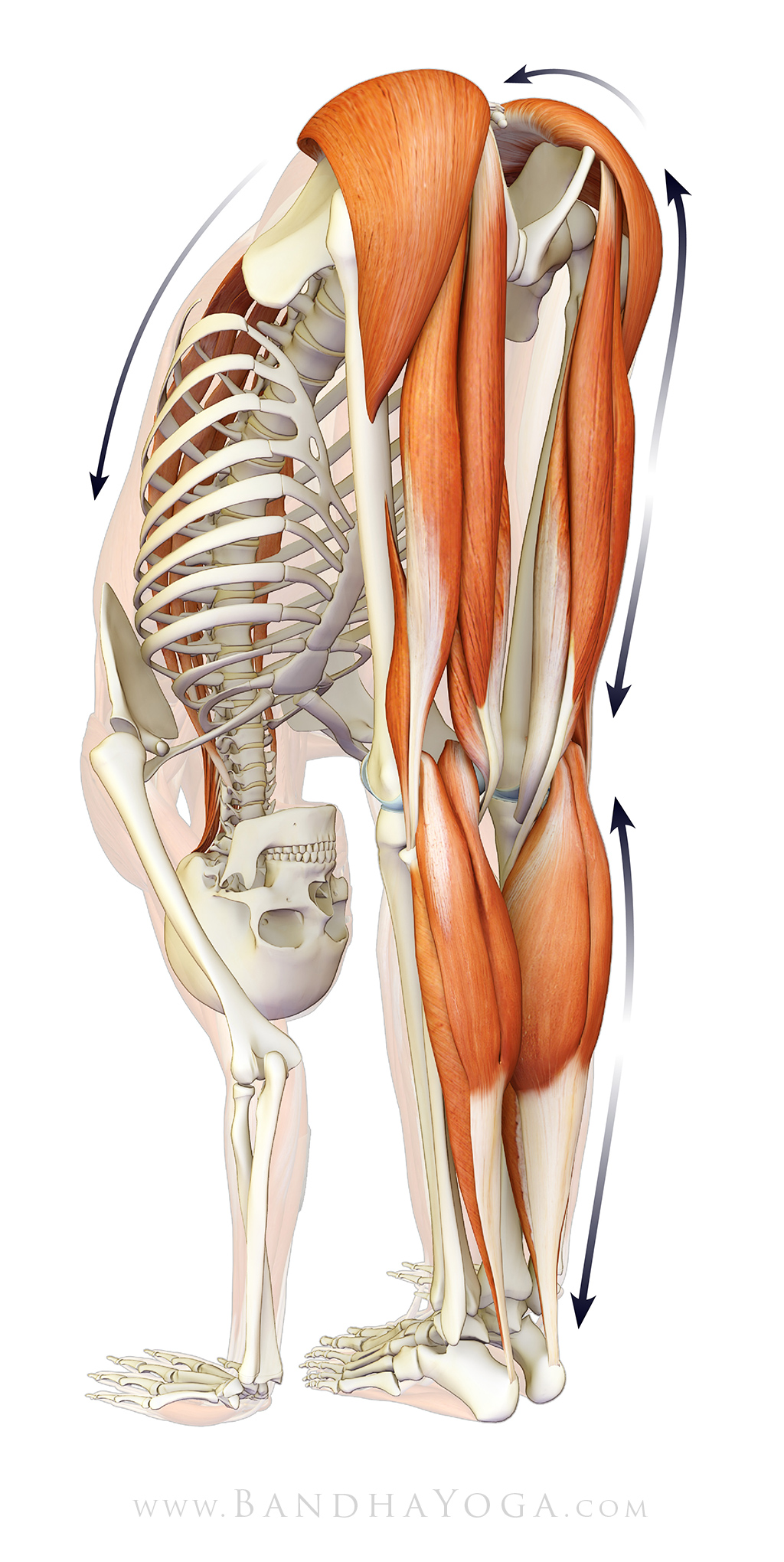
Once you get the hang of this cue in seated angle pose, try it in other forward bends like Janu sirsasana (figure 5). This illustrates the concept of “portability” for these cues. For many more similar tips, check out the Yoga Mat Companion book series. Learn about the individual muscles in the context of yoga from The Key Muscles and Key Poses of Yoga (you can use the "page through" feature to see the entire books).
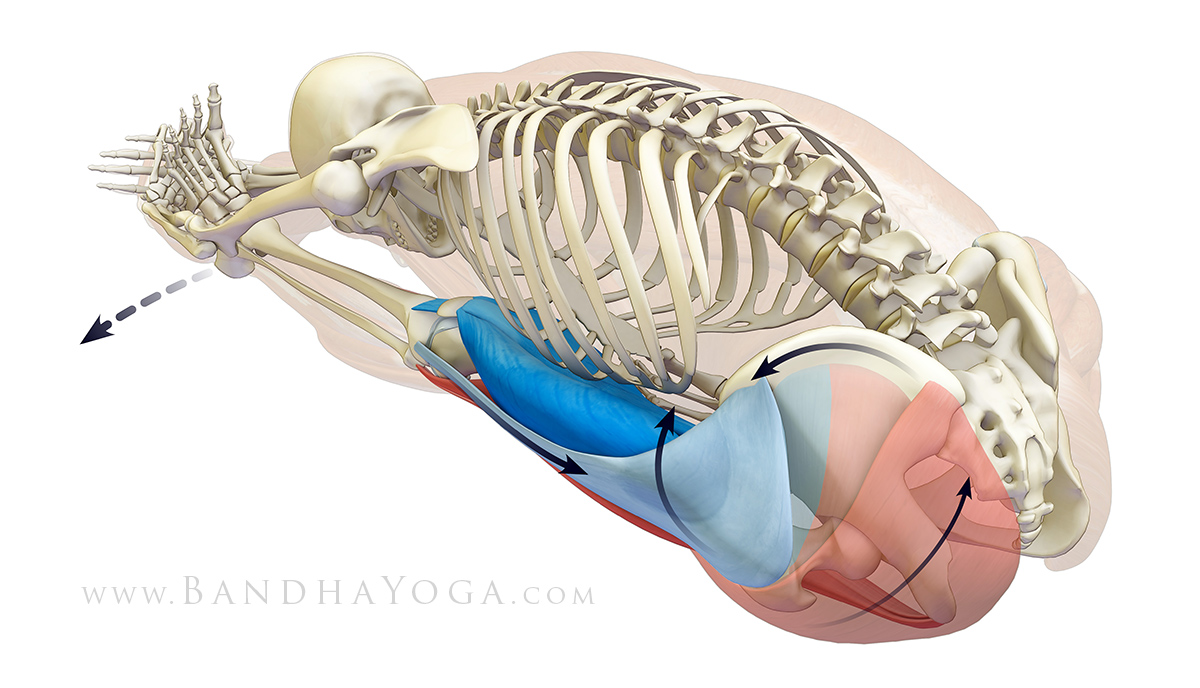 |
| Figure 5 illustrates the action of the TFL on tilting the pelvis forward, internally rotating the thighs and synergizing the quadriceps to extend the knees in Janu sirsasana. |
If you would like to learn more about combining modern Western science with the ancient art of yoga, please join us for a week in paradise at Blue Spirit Costa Rica for our second annual intensive on anatomy, biomechanics and therapeutics for Hatha yoga. I will be teaching state of the art techniques on these subjects, including much new material relating to therapeutic applications of yoga--all with great 3-D illustrations, excellent food, beautiful facilities and expertly taught daily Hatha yoga classes. We encourage you to register soon, as this workshop is nearly full.
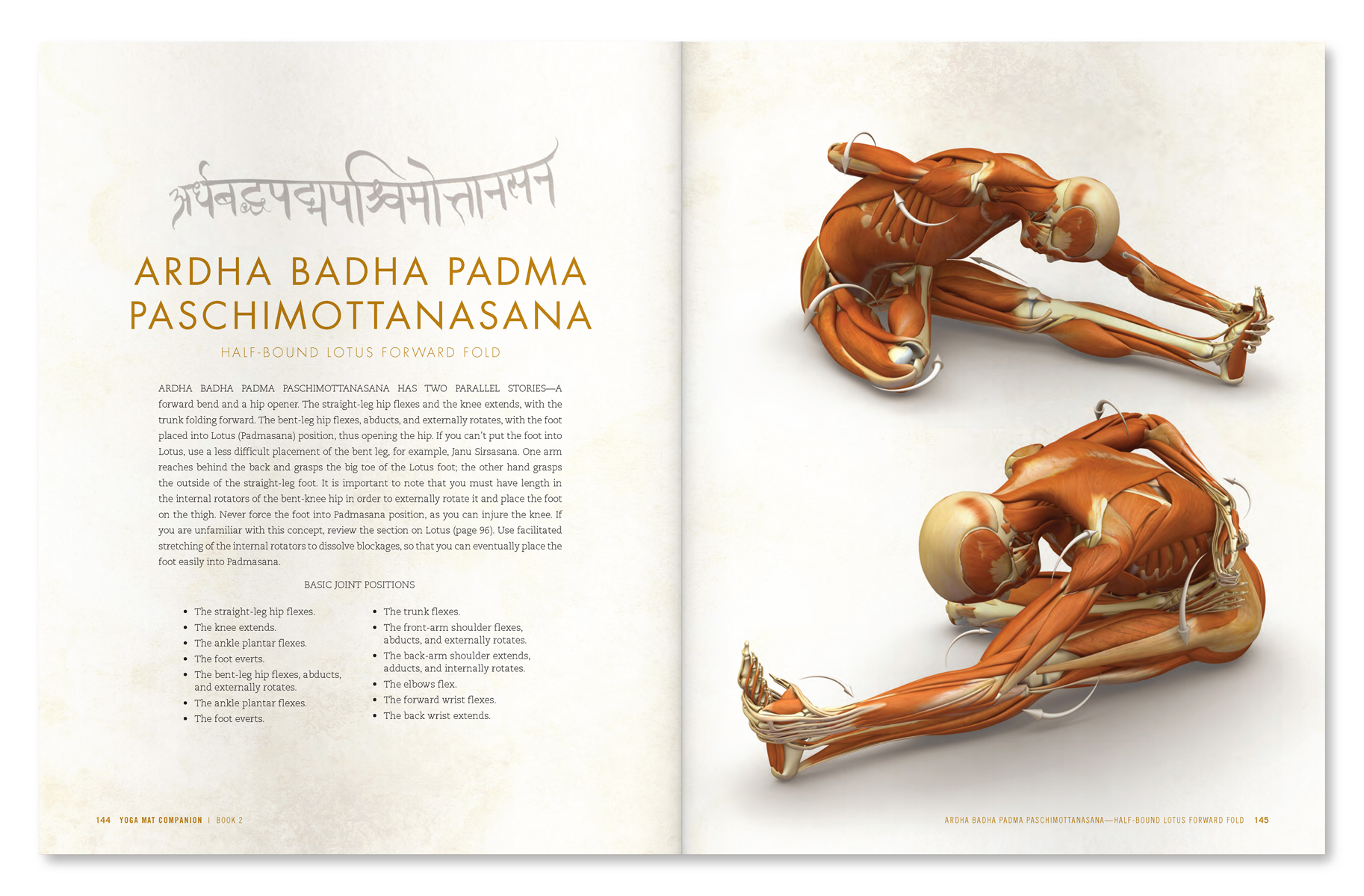 |
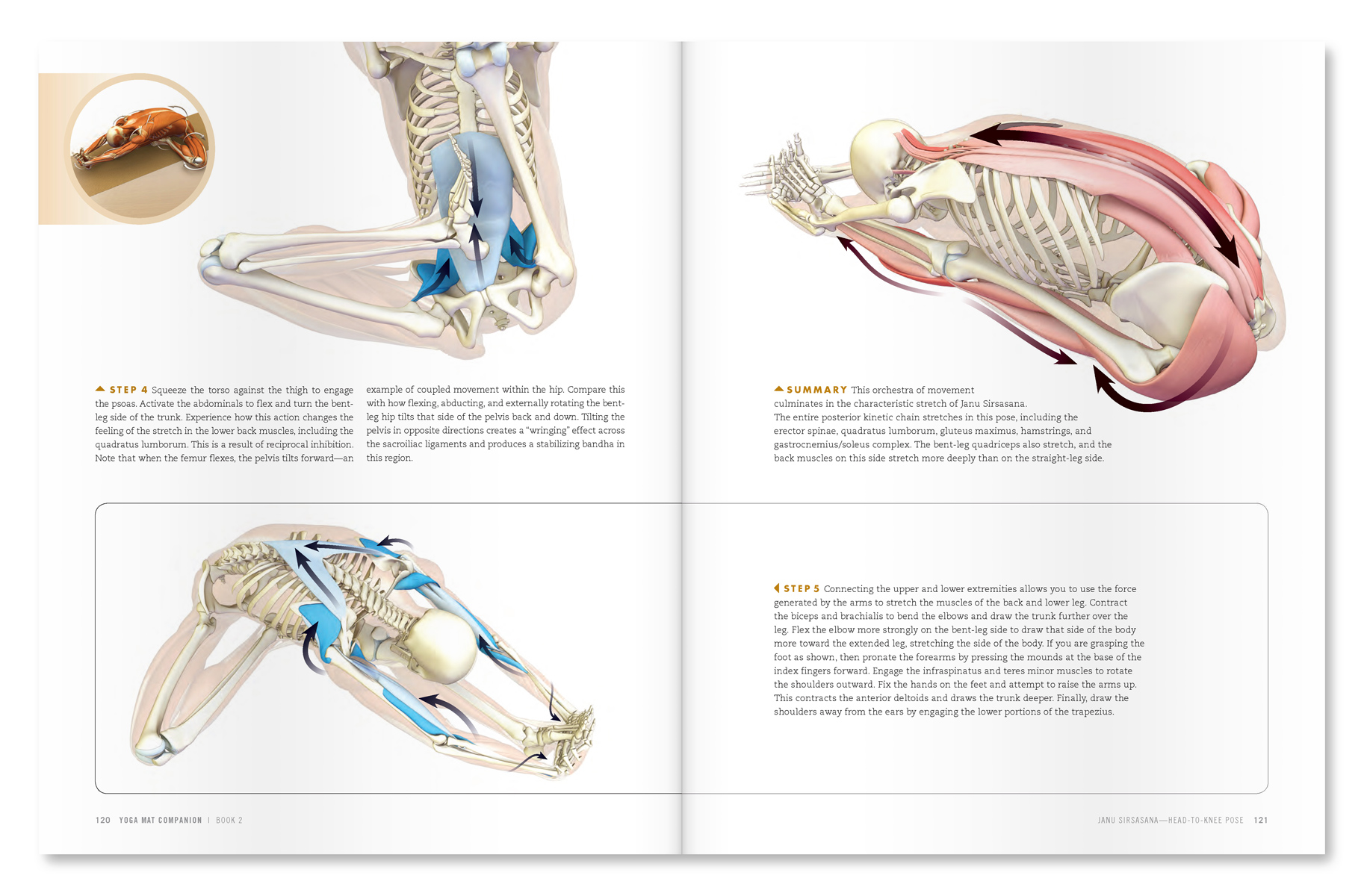
| An excerpt from "Yoga Mat Companion 2 - Anatomy for Hip Openers and Forward Bends". |
 |
| An excerpt from "Yoga Mat Companion 2 - Anatomy for Hip Openers and Forward Bends". |
Thanks for stopping by the Daily Bandha. Stay tuned for our next post when I'll go over a common condition affecting the shoulder joint and its yoga solution. Also, we greatly appreciate when you share us on Facebook, Twitter and Google Plus.
Namaste'
Ray and Chris