
In this post we discuss labral tears and the condition of joint hypermobility. I also present the case of a specific injury from yoga practice, its biomechanical basis and the steps that can be taken to aid in its prevention.
First, however, let’s look at the concept of association vs causality. Simply put, because some activity is associated with a problem does not mean it caused it. In medicine, when we recognize that an injury is associated with a specific activity we then investigate whether there are factors associated with that activity that could cause the injury. An example would be anterior cruciate ligament (ACL) tears.
A while back, we recognized that ACL tears were approximately five times more common in female athletes compared to males. Thus, investigators sought to identify circumstances that could account for this increased incidence. The risk factor thought to contribute most significantly to the higher rate of ACL ruptures in female athletes related to insufficient neuromuscular control of the knee joint in certain athletes. Accordingly, neuromuscular training regimens were devised that have reduced the incidence of ACL ruptures in this group. This approach to ACL injuries is an example of working with science to decrease the risk of an activity, not the activity itself. With this in mind, let’s look at the potential association of joint hypermobility with yoga injuries.
A while back, we recognized that ACL tears were approximately five times more common in female athletes compared to males. Thus, investigators sought to identify circumstances that could account for this increased incidence. The risk factor thought to contribute most significantly to the higher rate of ACL ruptures in female athletes related to insufficient neuromuscular control of the knee joint in certain athletes. Accordingly, neuromuscular training regimens were devised that have reduced the incidence of ACL ruptures in this group. This approach to ACL injuries is an example of working with science to decrease the risk of an activity, not the activity itself. With this in mind, let’s look at the potential association of joint hypermobility with yoga injuries.
Joint hypermobility, also known as generalized ligamentous laxity, is a spectrum ranging from mild “loose joints” to systemic pathological conditions such as Ehlers Danlos syndrome (a rare inherited condition that affects the connective tissue throughout the body). “Benign” joint hypermobility, or “double jointedness”, affects between 5% and 15% of the population, with most studies showing this condition to be significantly more common in women vs men. We evaluate the degree of hypermobility using the Beighton criteria, which examines factors such as knee, elbow and thumb hyperextension. Based on these factors, a score is created to quantify whether a person has hypermobility syndrome.
Joint hypermobility affects the capsular and ligamentous stabilizers of the articulations, which are lax. It is associated with an increased incidence of musculoskeletal injuries, including to the labrum of the shoulder and hip joints due to increased translations across the structure. The mainstay of management for ligamentous laxity (hypermobile joints) is physical therapy that is focused on strengthening the muscular stabilizers surrounding a given joint and improving proprioception. Now, let’s look at joint hypermobility in relation to injuries that may be associated with yoga.
Injuries that can be unequivocally directly attributed to practicing yoga, like the one described below, are infrequent (in my clinical experience) simply because yoga practitioners are active people who engage in other pursuits that may also cause injuries (sports, dance etc). Put another way, folks that actually practice yoga are generally not couch potatoes. Further complicating the issue are age related disease processes that can affect the joints whether or not one practices yoga. Nevertheless, we need to watch for associations of injuries with yoga and, where possible, determine their underlying cause, identify subgroups that may be at particular risk, and take steps to minimize those risks. With this in mind, let’s look at a specific injury that was caused during yoga practice, its biomechanical basis and steps that can be taken to aid in prevention.
During the past year I saw one yoga injury that was specifically caused by practicing a pose. This involved an experienced teacher who was demonstrating the “wrong way” to perform Vasisthasana (side plank pose) by having the hand of the supporting arm forward of the shoulder joint instead of directly below the shoulder and at a right angle to the floor. In the process, she experienced a “clunk” in her shoulder, followed by pain. On exam in the clinic, she was found to have joint hypermobility, as quantified by the Beighton criteria. Her MRI demonstrated a tear of the posterior part of the shoulder labrum. Conservative treatment with physical therapy, etc. was not successful in relieving her pain and she required arthroscopic repair of the labrum with tightening of the capsule.
It is worth noting that this teacher had practiced Vasisthasana many times with the hand placed below the shoulder without difficulty. Additionally, on questioning it was clear that she was not actively engaging the muscular stabilizers of the shoulder joint during the demonstration.
Now, let’s look at the mechanism of injury. First, as part of their joint hypermobility, this person had a condition known as “multidirectional shoulder instability”. In patients with this condition, the shoulder capsule and ligaments are lax and thus, do not contribute sufficiently to stability of the joint. As a result, the head of the shoulder can “slide” around on the glenoid (socket) more than usual. This causes increased translational forces across the glenoid labrum. In this particular case, while attempting side plank, she subluxed the head of the humerus over the labrum, tearing it.
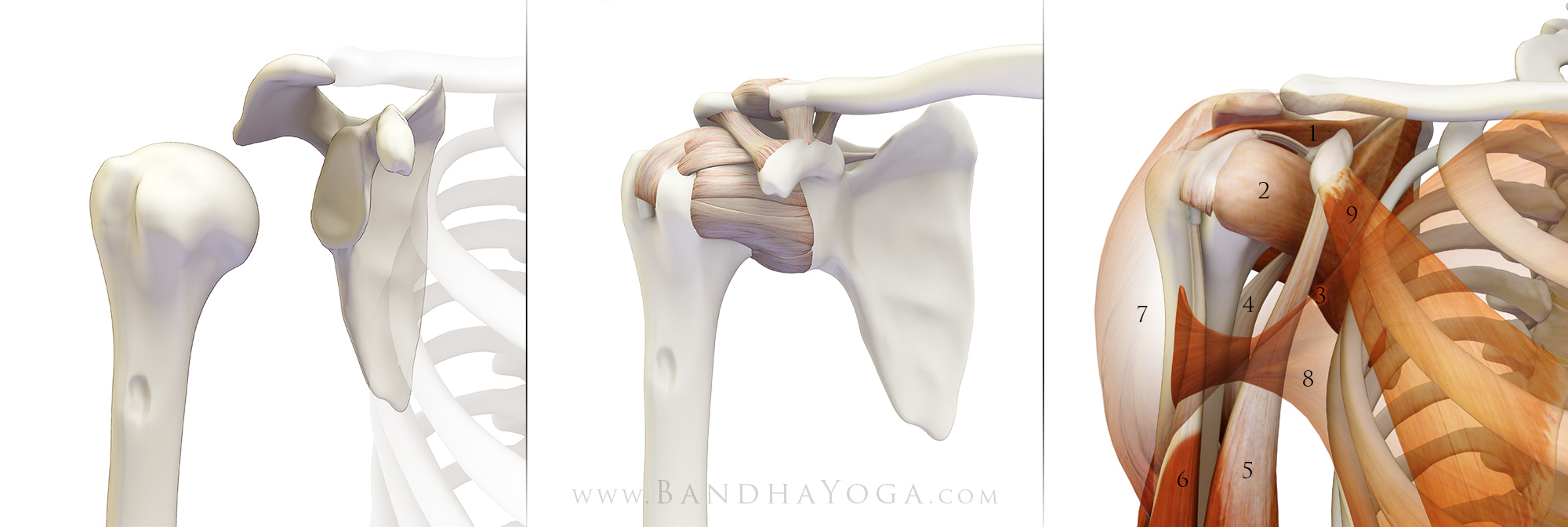 |
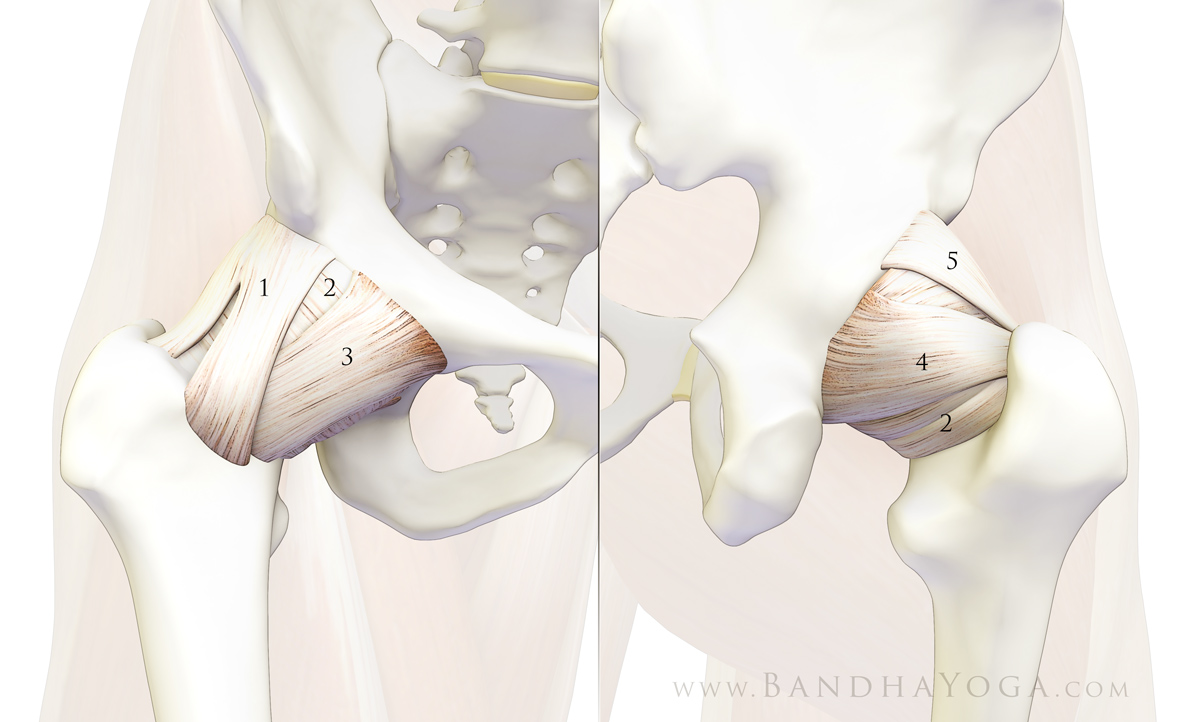
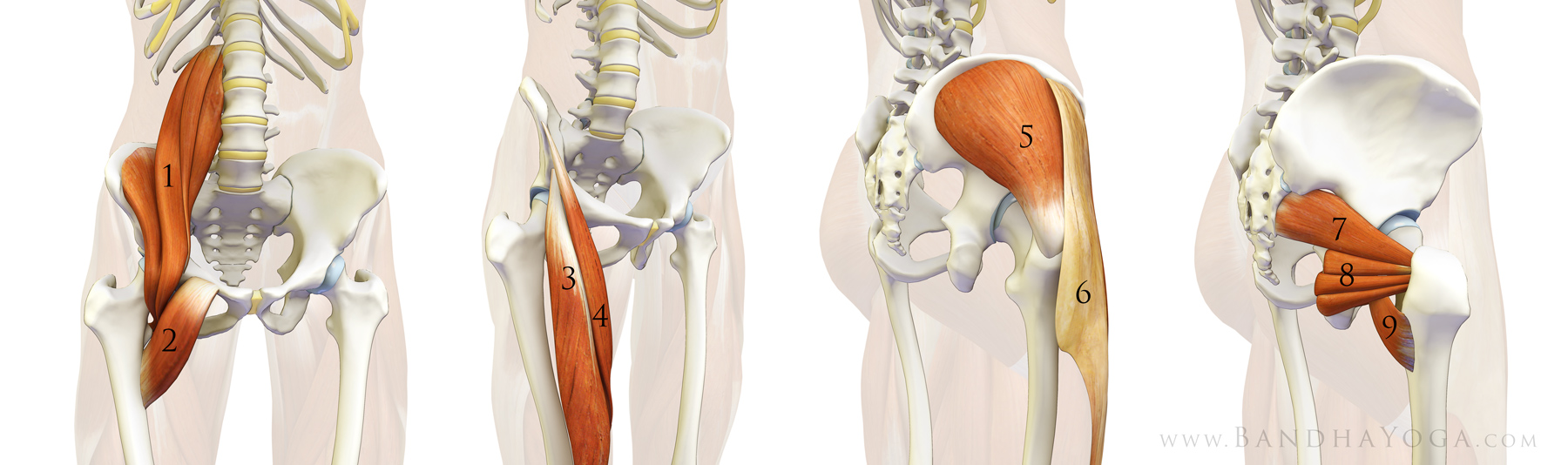
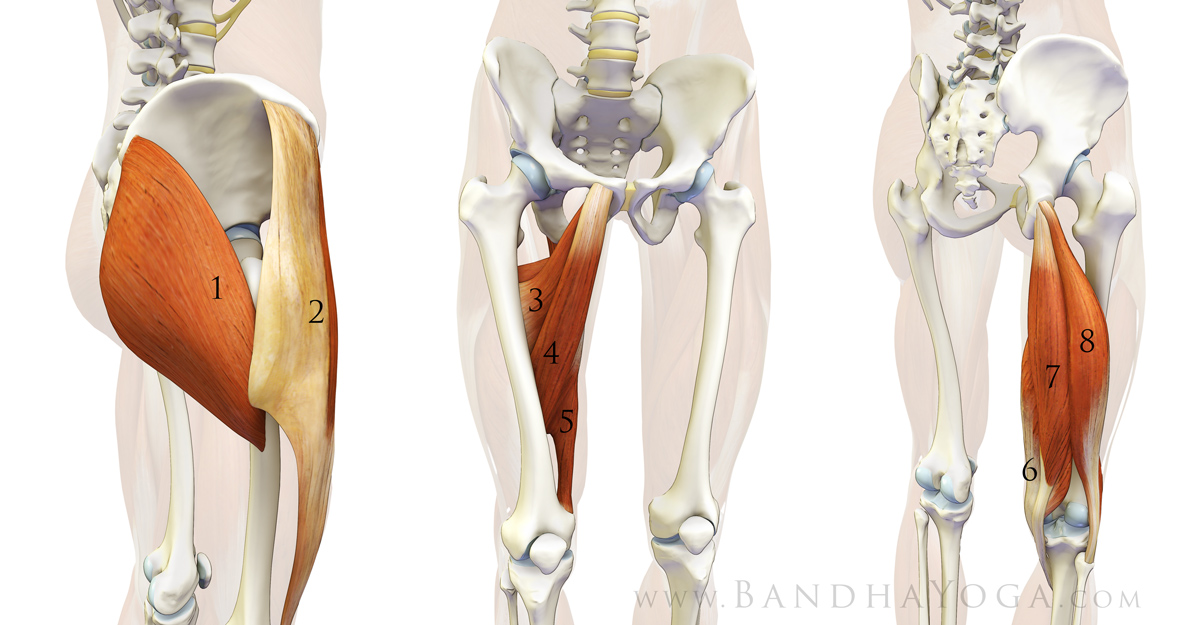
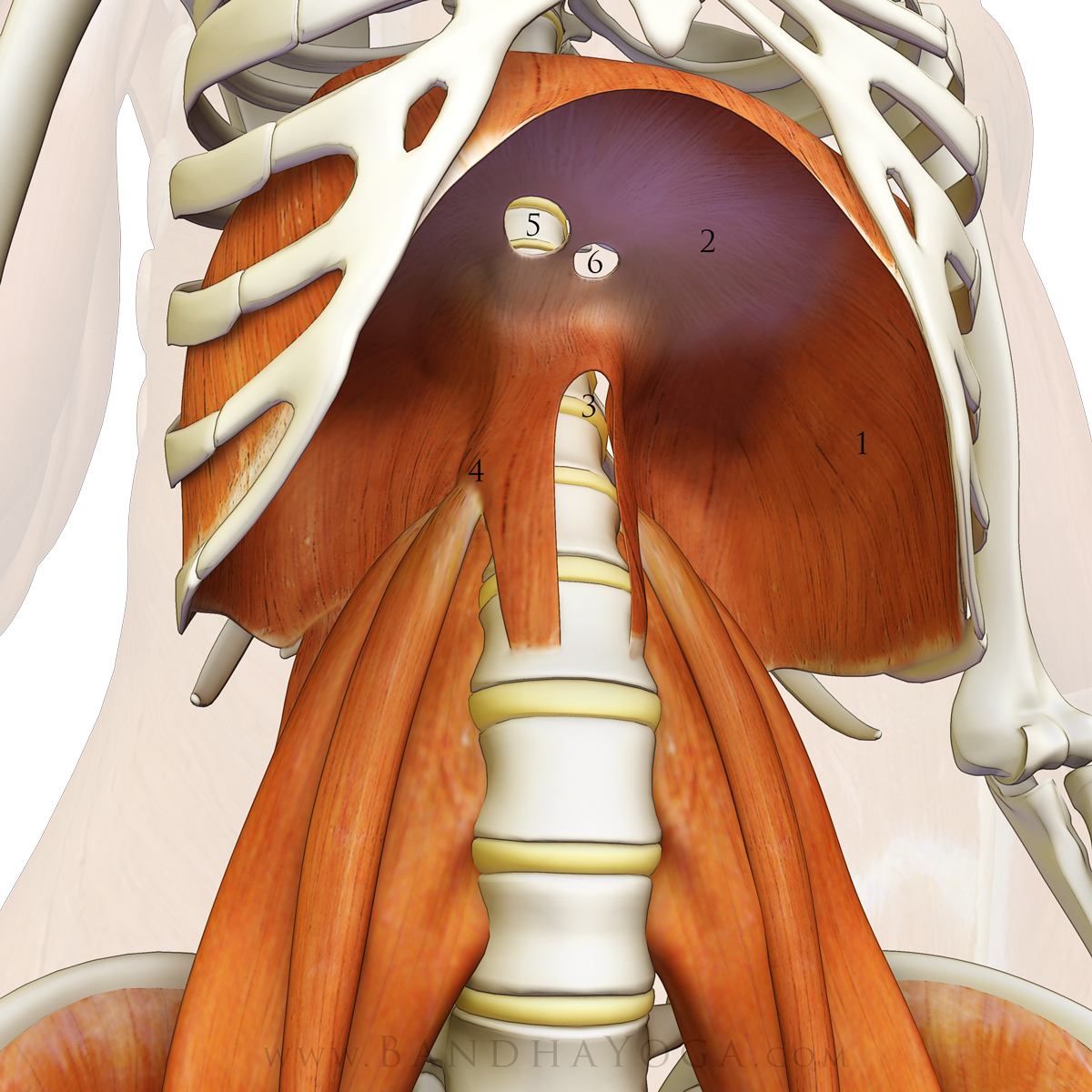
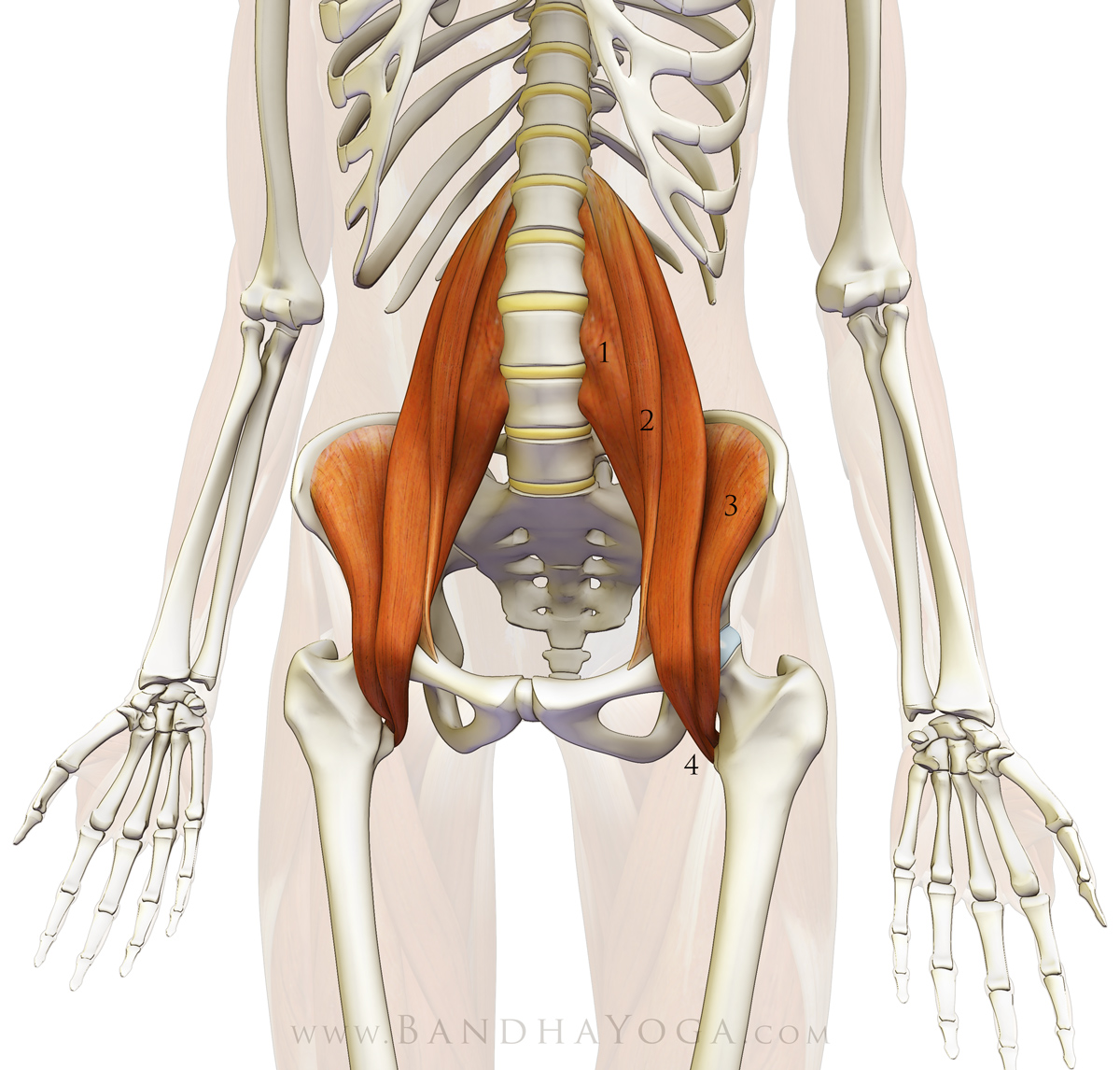
| Figure 1: Bone structure of the shoulder; Figure 2: Ligaments and capsule; Figure 3: Muscular stabilizers 1-supraspinatus, 2-subscapularis, 3-infraspinatus, 4-triceps, 5-biceps(short head), 6-biceps(long head), 7-deltoid, 8- pectoralis major, 9-pectoralis minor |
The three factors that contribute to mobility and stability of the joint are the bone shape, the capsulo-ligamentous structures and the muscles surrounding the articulation. Figure 1 illustrates the structure of the shoulder joint. Composed of a shallow socket and relatively thin capsular and ligamentous supports, this is the most mobile articulation in the body. The muscular stabilizers, including the rotator cuff play an important role in maintaining the congruency of the shoulder joint. When the capsule and ligaments are loose, then the muscles must compensate. This is why we focus on strengthening the muscles in multidirectional shoulder instability. Figures 1, 2 and 3 illustrate the bone structure, capsulo-ligamentous stabilizers and muscular stabilizers respectively.
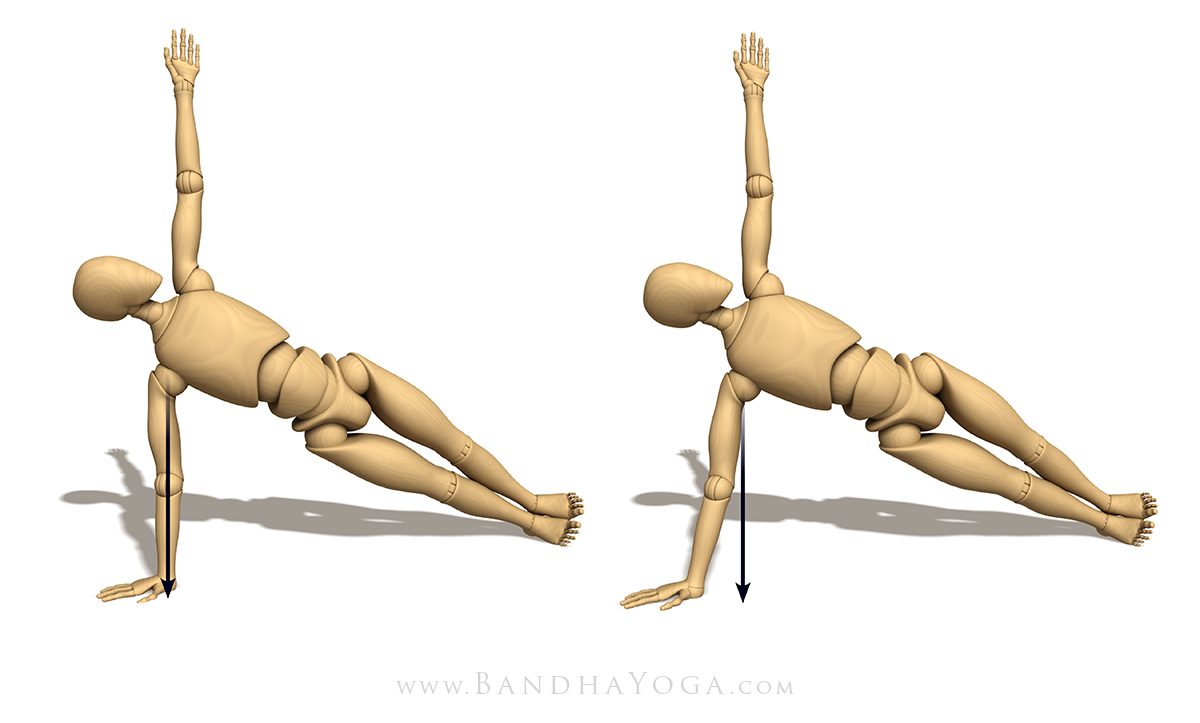 |
| Figure 4: Vasisthasana illustrating the direction of gravity in variations of hand position. |
Looking at the factors that caused this teacher to experience a subluxation with the hand forward of the shoulder we can see that, in this position, the body weight is directed at an angle to the alignment of the arm bones. When the hand is placed below the shoulder, the supporting arm is aligned in a position such that the bones are perpendicular to the direction of gravity. Practicing the pose in this way requires less muscular effort because it uses the inherent passive strength of the bones to aid in supporting the body weight. When the hand is placed forward of the shoulder, greater muscular effort is required to maintain the pose (figure 4).
People with joint hypermobility depend to a greater degree on the muscular stabilizers of the joint. Placing the hand so that the arm is angled against gravity means that these muscles must also work to support the body weight that would be borne, in part, by the bones. You can experience this concept yourself by standing near a wall and leaning against it (figure 5). Then, move the feet a bit further from the wall. Which one requires less muscular effort?
 |
| Figure 5: Illustrating using bone alignment vs muscular force. |
Figures 6 illustrates Vasisthasana with the supporting muscular stabilizers. I go over a step-wise approach to engaging these muscles and the other core stabilizers of the trunk and legs in Yoga Mat Companion Four (arm balances and inversions).
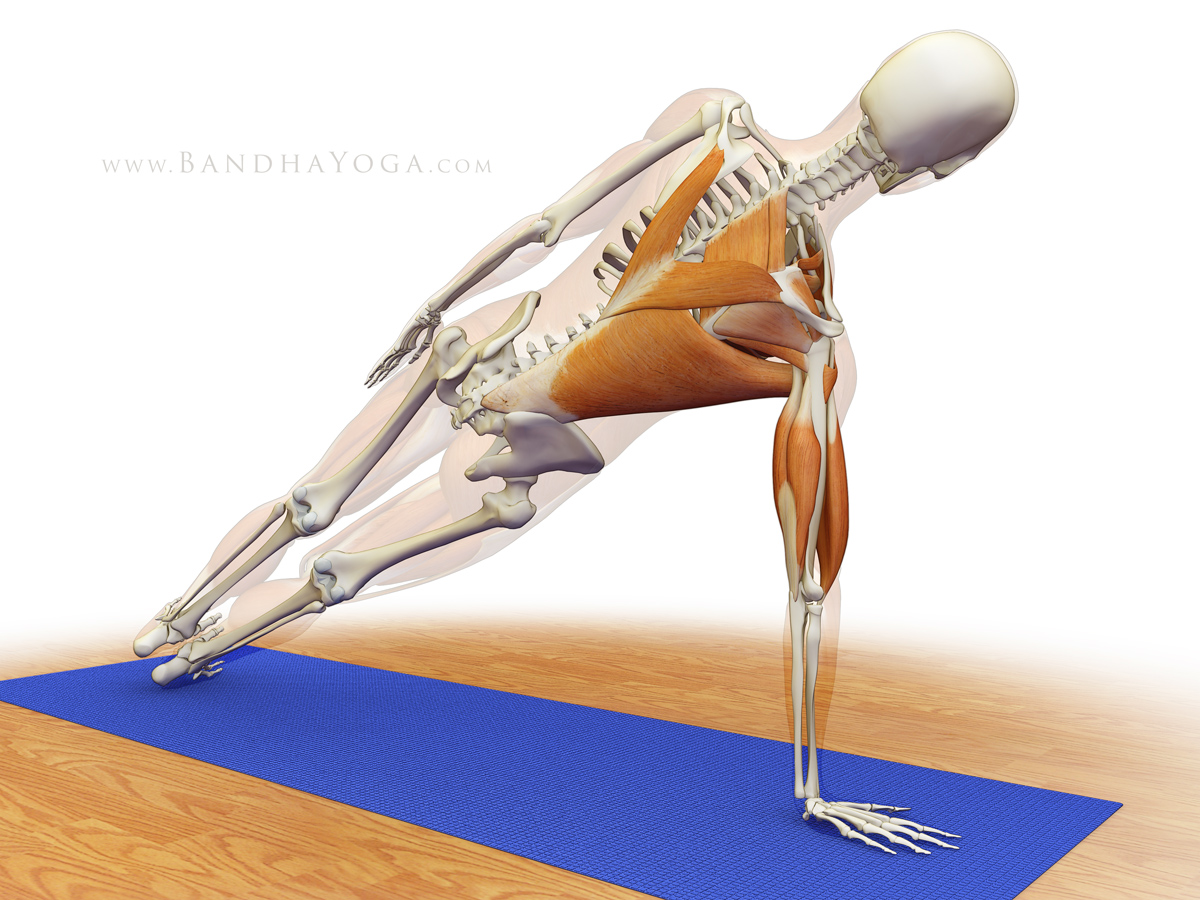 |
| Figure 6: Muscular stabilizers of the shoulder in Vasisthasana. |
Labral Tears in the Hip:
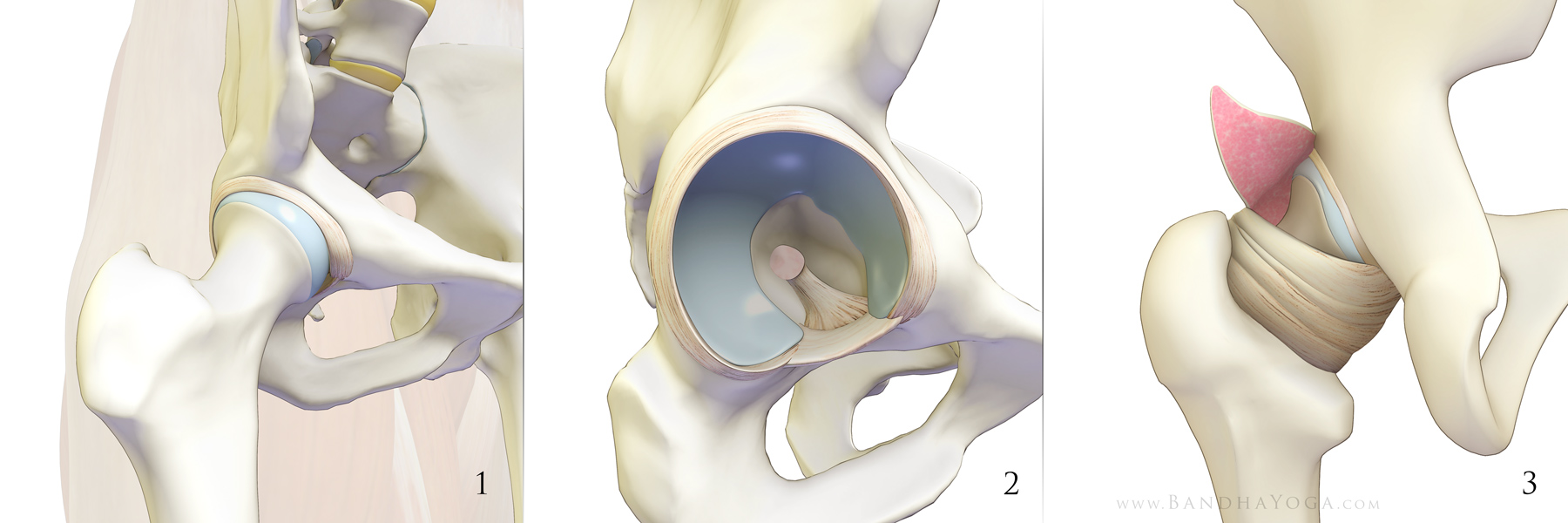
In our most recent blog post we discussed the normal structure and function of the hip labrum. Now let’s discuss labral tears. A number of activities have been associated with this injury including soccer, hockey, golf, ballet, gymnastics, and running. Additionally, a number of specific movements have been associated with labral tears. Pregnancy and childbirth have also been associated with acute tears of the labrum. Even shopping has been associated with injuries to this structure ("supermarket hip"). Other causes of labral tears include ligamentous laxity and abnormalities of the bone. Nevertheless, up to 75% of the time, symptomatic labral tears of the hip are not associated with an identifiable event or cause.
Adding to the complexity is the consideration that labral pathology may be related to the aging process, with up to 96% of cadaver specimens having tears. Furthermore, labral tears do not always cause pain; indeed, a prospective blinded study published in the American Journal of Sports Medicine identified labral tears in 69% of the joints studied in volunteers with no history of injury, pain or other symptoms. Even accounting for false positive mri’s, that is a significant number. Hip injuries and arthritis are among the most intensively investigated areas in medicine today, with new studies being published each month. In this regard, please review the linked references below.
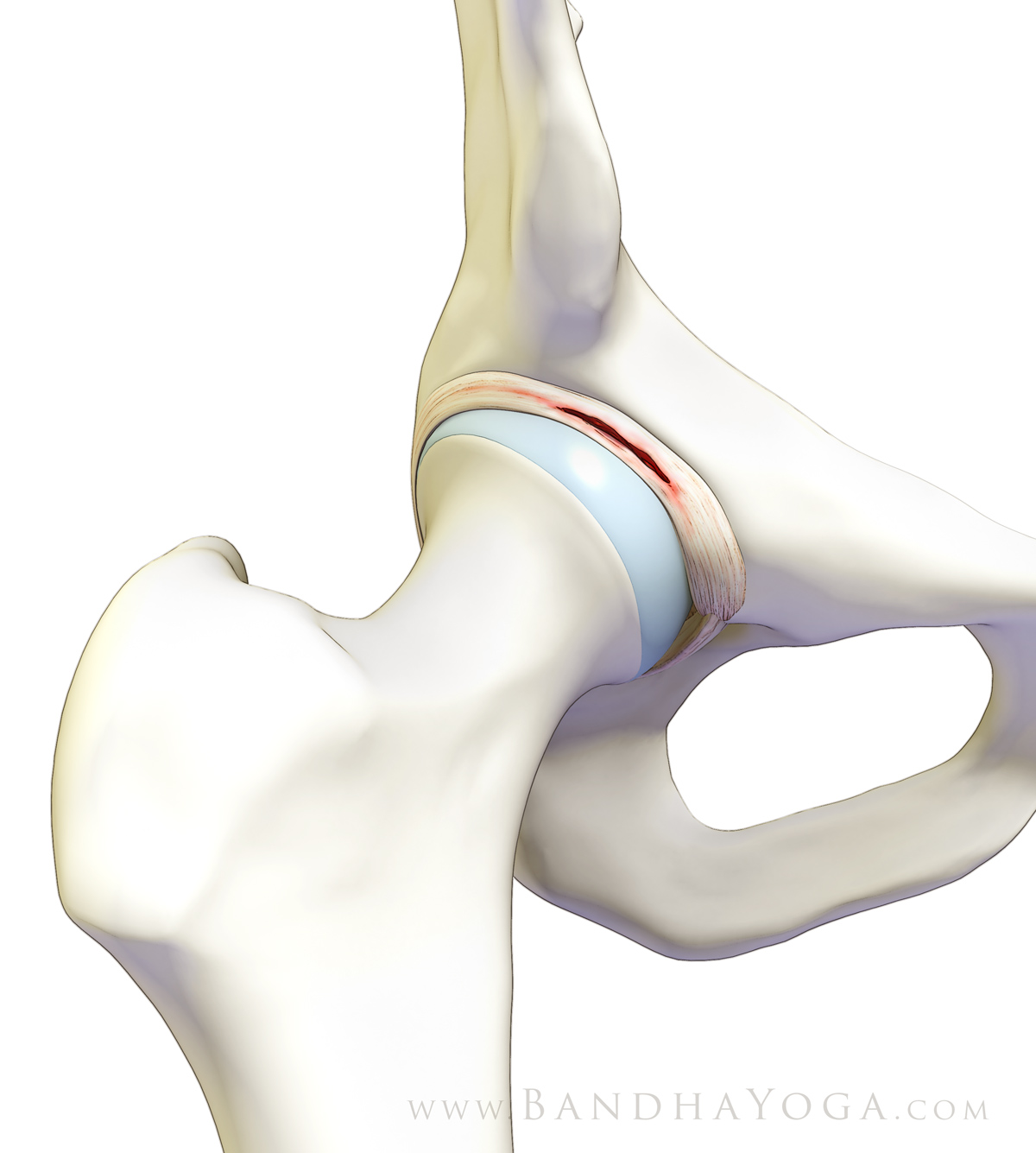 |
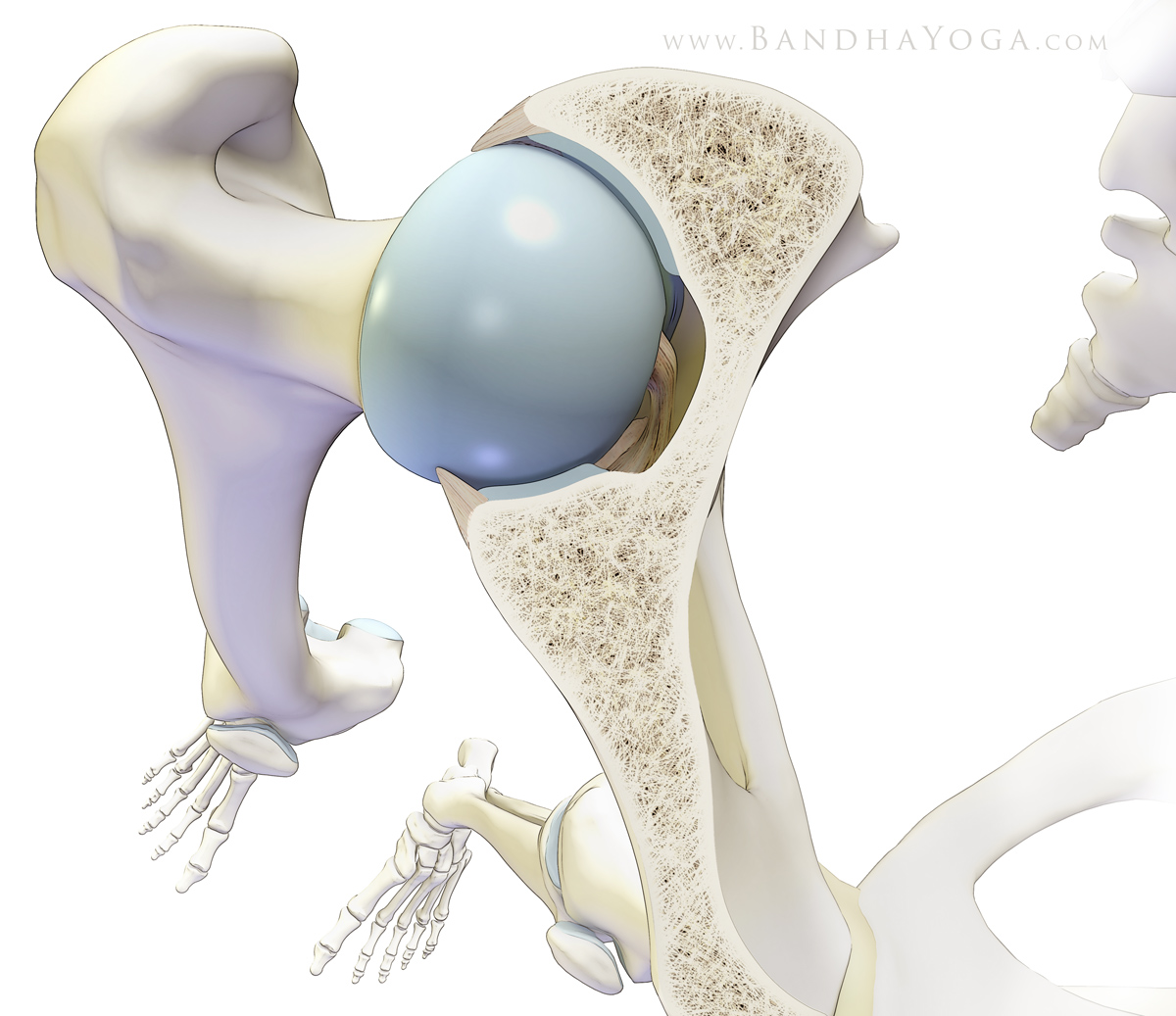
| Figure 7: Hip Labral Tear. |
One of the known causes of tears of the hip labrum is joint hypermobility. This is also a factor during pregnancy, when hormonal influences cause ligamentous laxity in persons who are not normally hypermobile. Tears of the hip labrum occur in this setting as result of increased translational forces across the labrum from the femoral head. As with hypermobile joints elsewhere in the body, hypermobility in the hips is managed (at least initially) by strengthening the muscular stabilizers that surround the joint. This aids to prevent injuries.
I think this is relevant in light of recent media attention on hip injuries and yoga, particularly since many of those practicing poses that take the hip joints into extreme positions also have hypermobile joints. In my experience, such individuals—who can easily perform extreme movements—often do so without maintaining muscular engagement during extremes of motion. Of particular note is a recent NY Times article that discusses flexibility as a liability for women in yoga. While spending considerable time discussing bone abnormalities (which are more prevalent in men, and were not thought to be a factor in studies on dancers), the NY Times article does not discuss joint hypermobility or the use of muscular stabilization during practice--something that is a cornerstone of injury prevention, especially in persons with high levels of joint mobility. Perhaps a more relevant view of the matter was presented in the Canadian media.
Finally, here are a couple of suggestions that I have found to be helpful in my own practice and teaching:
- Ease into the end points of poses. Joints adapt to gradual changes much better than abrupt or rapid ones. For example, I deliberately slow down my movement as I near the end point of forward flexion in Uttanasana. This helps to protect the joints and also creates mindfulness in the practice.
- Use gentle muscular engagement to stabilize the joints. This is a cornerstone of rehabilitation and injury prevention. Knowledge of the musculoskeletal system and visualization helps in this process.
Note: if you have hip pain or other symptoms (from any activity), be sure to consult a health care professional who is appropriately trained and qualified to diagnose and manage such conditions. Follow their guidelines for your condition.
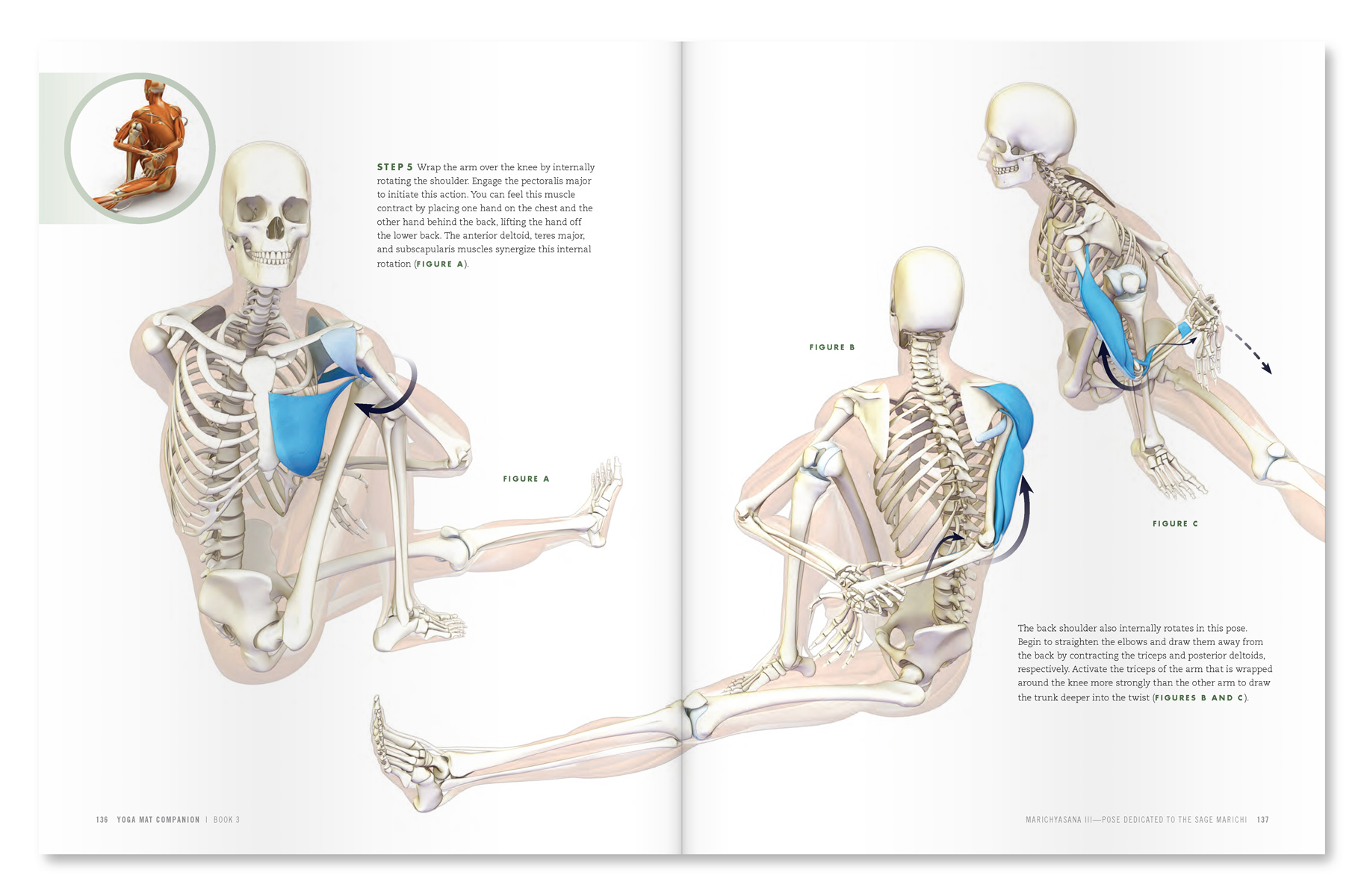 |
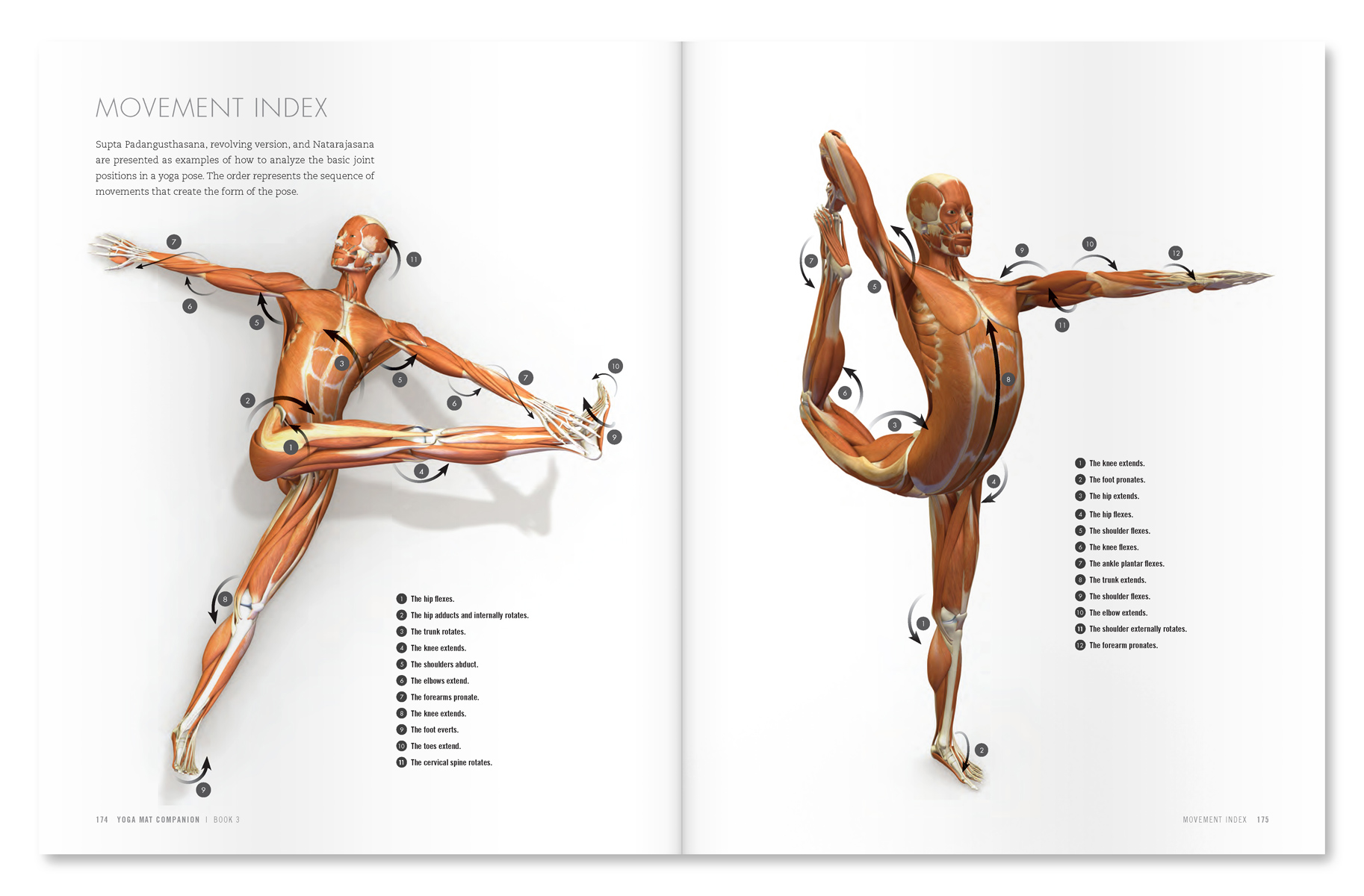
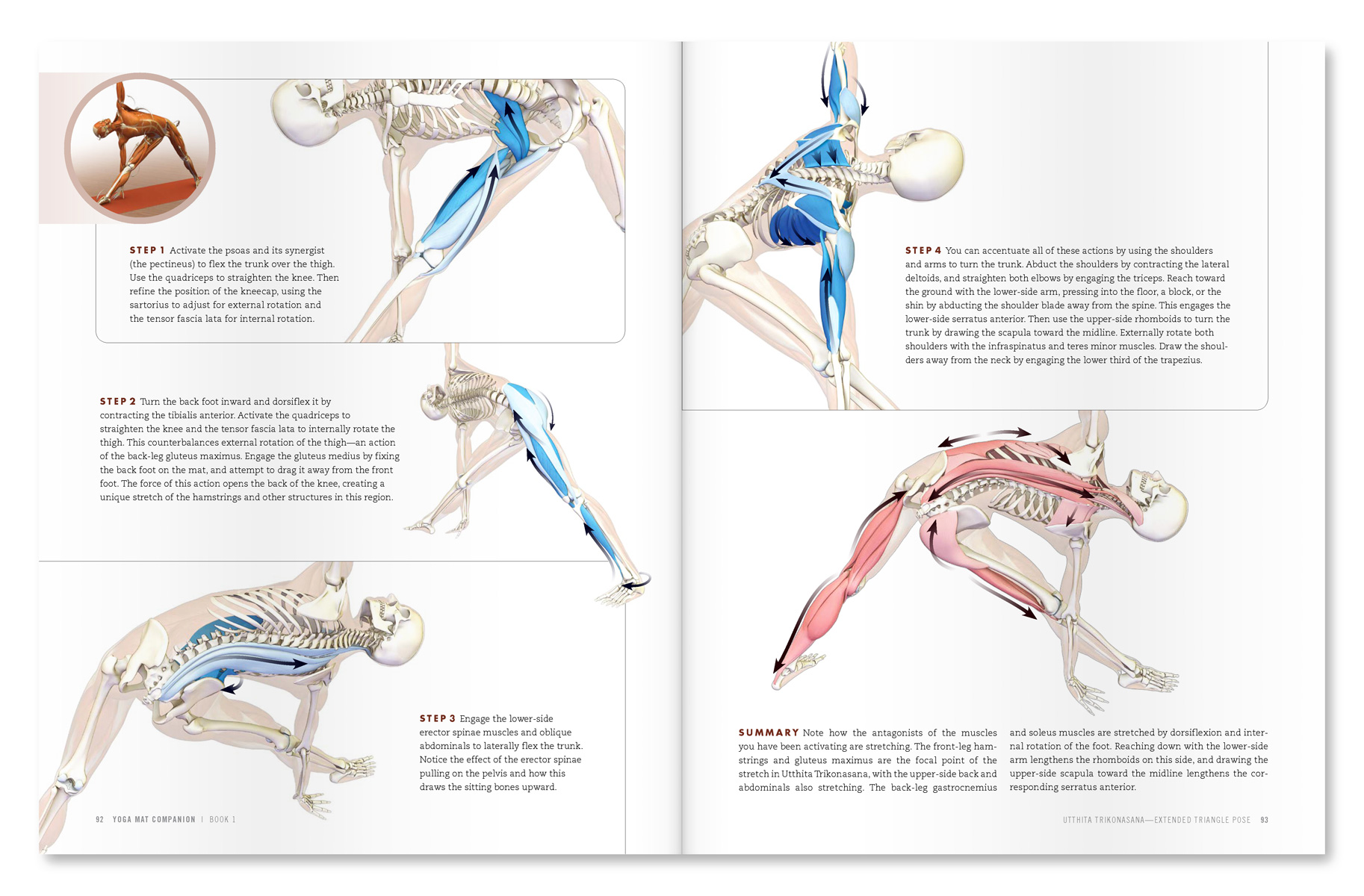
| An excerpt from "Yoga Mat Companion 3 - Anatomy for Arm Backbends and Twists". |
 |
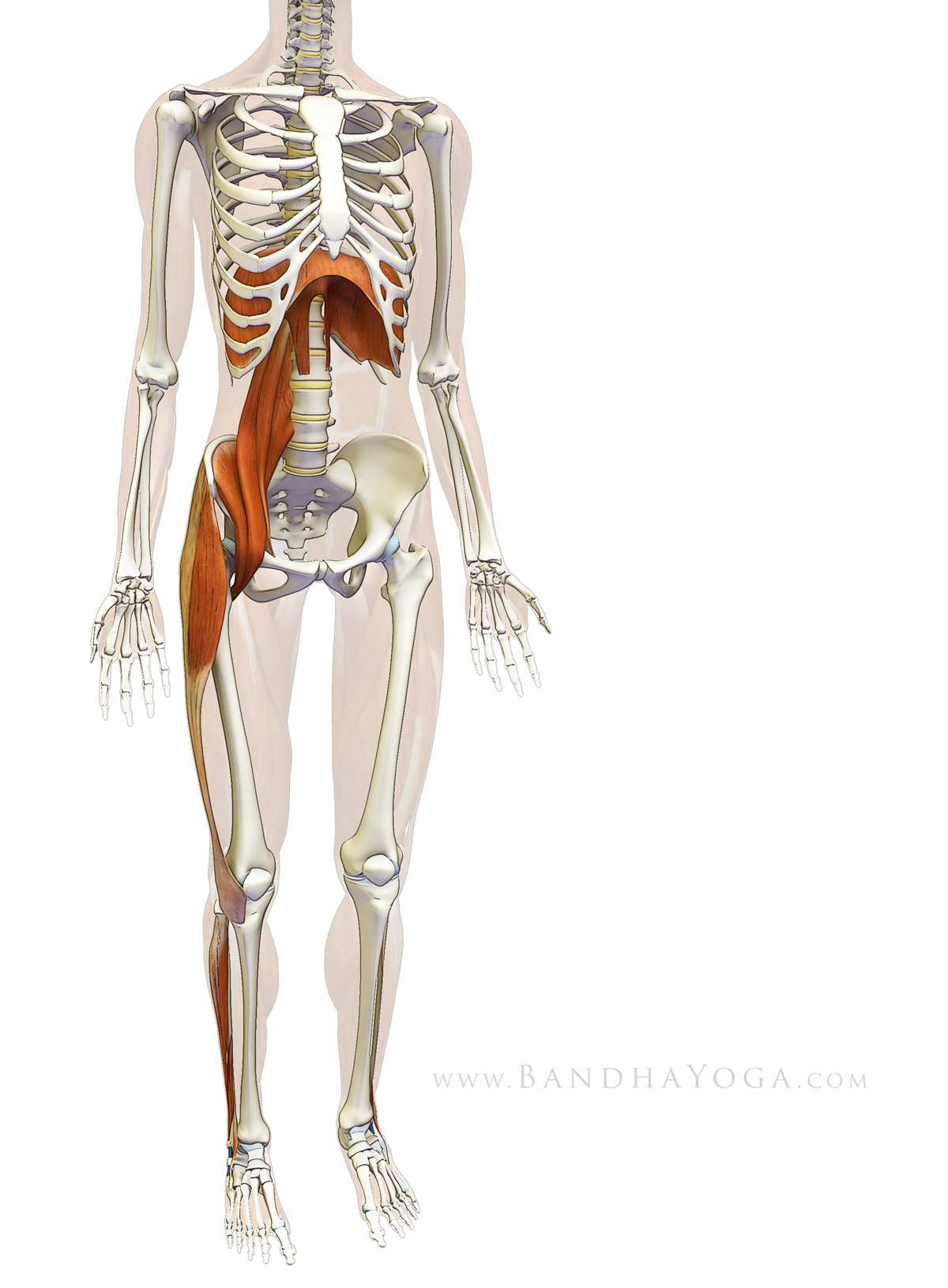
| An excerpt from "Yoga Mat Companion 4 - Anatomy for Arm Balances and Inversions". |
To learn more about anatomy, biomechanics and yoga, feel free to page through The Key Muscles and Key Poses of Yoga and the Yoga Mat Companion Series.
All the Best,
Ray Long, MD
References:
- Mandelbaum BR, Silvers HJ, Watanabe DS, Knarr JF, Thomas SD, Griffin LY, Kirkendall DT, Garrett W Jr. “Effectiveness of a neuromuscular and proprioceptive training program in preventing anterior cruciate ligament injuries in female athletes: 2-year follow-up.” Am J Sports Med. 2005 Jul;33(7):1003-10.
- Wolf JM, Cameron KL, Owens BD. “Impact of joint laxity and hypermobility on the musculoskeletal system.” J Am Acad Orthop Surg. 2011 Aug;19(8):463-71.
- Pacey V, Nicholson LL, Adams RD, Munn J, Munns CF. “Generalized joint hypermobility and risk of lower limb joint injury during sport: a systematic review with meta-analysis.” Am J Sports Med. 2010 Jul;38(7):1487-97.
- Konopinski MD, Jones GJ, Johnson MI. “The effect of hypermobility on the incidence of injuries in elite-level professional soccer players: a cohort study.” Am J Sports Med. 2012 Apr;40(4):763-9.
- McCormack M, Briggs J, Hakim A, Grahame R. “Joint laxity and the benign joint hypermobility syndrome in student and professional ballet dancers.” J Rheumatol. 2004 Jan;31(1):173-8.
- Boykin RE, Anz AW, Bushnell BD, Kocher MS, Stubbs AJ, Philippon MJ. “Hip instability.” J Am Acad Orthop Surg. 2011 Jun;19(6):340-9.
- Lewis CL, Sahrmann SA. “Acetabular labral tears.” Phys Ther. 2006 Jan;86(1):110-21.
- Groh MM, Herrera J. “A comprehensive review of hip labral tears.” Curr Rev Musculoskelet Med. 2009 Jun;2(2):105-17.
- Baker JF, McGuire CM, Mulhall KJ. “Acetabular labral tears following pregnancy.” Acta Orthop Belg. 2010 Jun;76(3):325-8.
- Yamamoto Y, Villar RN, Papavasileiou A. “Supermarket hip: an unusual cause of injury to the hip joint.” Arthroscopy. 2008 Apr;24(4):490-3
- Register B, Pennock AT, Ho CP, Strickland CD, Lawand A, Philippon MJ. “Prevalence of abnormal hip findings in asymptomatic participants: a prospective, blinded study.” Am J Sports Med. 2012 Dec;40(12):2720-4.
- Agricola R, Heijboer MP, Roze RH, Reijman M, Bierma-Zeinstra SM, Verhaar JA, Weinans H, Waarsing JH. “Pincer deformity does not lead to osteoarthritis of the hip whereas acetabular dysplasia does: acetabular coverage and development of osteoarthritis in a nationwide prospective cohort study (CHECK).” Osteoarthritis Cartilage. 2013 Oct;21(10):1514-21.
- Leunig M, Jüni P, Werlen S, Limacher A, Nüesch E, Pfirrmann CW, Trelle S, Odermatt A, Hofstetter W, Ganz R, Reichenbach S. “Prevalence of cam and pincer-type deformities on hip MRI in an asymptomatic young Swiss female population: a cross-sectional study.” Osteoarthritis Cartilage. 2013 Apr;21(4):544-50.
- Agricola R, Heijboer MP, Bierma-Zeinstra SM, Verhaar JA, Weinans H, Waarsing JH. “Cam impingement causes osteoarthritis of the hip: a nationwide prospective cohort study (CHECK).” Ann Rheum Dis. 2013 Jun;72(6):918-23.
- Charbonnier C, Kolo FC, Duthon VB, Magnenat-Thalmann N, Becker CD, Hoffmeyer P, Menetrey J. “Assessment of congruence and impingement of the hip joint in professional ballet dancers: a motion capture study.” Am J Sports Med. 2011 Mar;39(3):557-66.




{kind=link}
{kind=link}